I. Introduction
Cloud computing-based desktop virtualization (i.e., virtual desktop infrastructure [VDI]) is a technology that enables access to a personal computer environment regardless of the connecting device, at any time or place that the Internet is available [1,2].
As the need for swift coordination between healthcare professionals of diverse disciplines and timely point-of-care access to information has grown in medical environments such as hospitals, the interest in establishing mobile healthcare environments has also grown [3,4]. VDI system allows the fast, organization-wide establishment of a mobile hospital environment without the need to modify the existing legacy clinical applications or to develop new mobile applications.
However, despite the interest in the emerging technology due to its advantages in terms of efficient management of physical resources and rapid service deployment [5-7], actual implementations are not yet common. A few recent studies showed the possible use of VDI for teleradiology [8] and emergency healthcare [9]. There are very few cases of the organization-wide establishment of a mobile hospital environment using VDI, and the concerns arising when establishing a mobile hospital environment and applying it in the field are not yet well understood.
Based on the establishment of an organization-wide mobile consultation environment, in which a VDI system was accessed through an iPad at a university hospital with 910 beds, this study examined the problems to be considered when implementing and utilizing VDI in a hospital in order to share our early experiences on the adoption of the emerging technology.
Additionally, in keeping with the paradigm shift to patient-centered medicine [10-15], the VDI-based mobile hospital environment was applied to physician's rounds as a case study for the use of VDI in patient care. The resulting patient satisfaction and the concerns experienced by the participated physicians regarding the mobile hospital environment were examined.
II. Methods
1. Study Site
This study was performed at the Seoul National University Bundang Hospital (SNUBH), located in the Seoul metropolitan area of South Korea. SNUBH is a tertiary national university hospital founded in May 2003 as a fully digital hospital. It was accredited with a Stage 7 of Electronic Medical Record (EMR) adoption model from the Healthcare Information and Management Systems Society (HIMSS) Analytics on October 2010 [16]. The hospital has 910 beds and was visited by an average of approximately 4,100 outpatients daily during 2011.
2. Implementation of Mobile Hospital Environment Using VDI
SNUBH launched VDI system in November 2011 after the system was implemented using VMware 5.0 over approximately 4 months, beginning in July 2011. The system was implemented so that the use of all hospital information systems, including clinical and administrative applications such as EMR, Picture Archiving Communication System (PACS) and groupware, was possible on all devices, including desktops, iOS-based tablet PCs, Android-based tablet PCs, and laptops. The system was concurrently accessible by 400 users.
Figure 1 shows the overall system architecture of VDI, consisting of virtual private networks (VPN), virtualization network, VDI servers, management and access servers, and storage area network (SAN) switches. The system architecture was established to achieve high availability and stability of the VDI service through dual implementation of all servers such as a management server, an access server, an active directory (AD) server, switch servers, and VPN. And, VDI server was clustered so that the virtualization service can function even with a 20% hardware failure.
In addition, in order to implement a mobile hospital environment an iPad was provided to every medical professor so that they can access VDI at anytime and anywhere.
3. Research Model for the Case Study of Mobile Consultation Service Using VDI
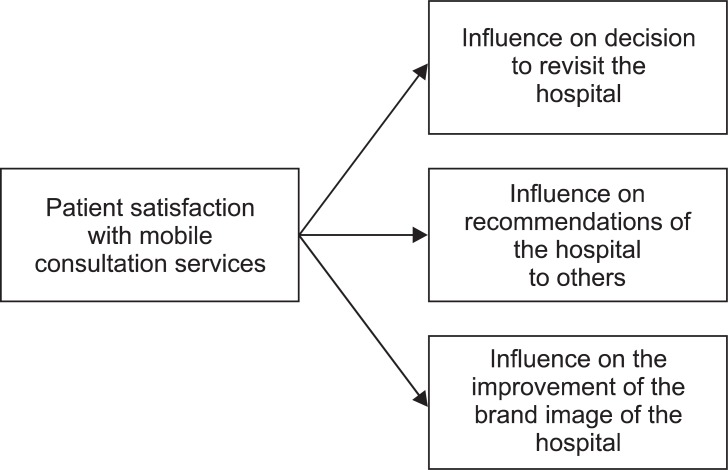
As a case study of using VDI for patient care, we surveyed the possible use of the system in physician's round. We examined the relationship between patient satisfaction with the point-of-care mobile consultation service, which used hospital information systems on a virtual desktop with an iPad, and 3 variables representing the influence of their experience on their likelihood of revisiting the hospital (labeled the revisit), on their likelihood of recommending the hospital to other people (labeled recommendation), and on whether they believed the service would help to improve the brand image of the hospital (labeled brand image) (Figure 2).
4. Study Subjects
A survey was conducted on the satisfaction of 35 inpatients and their next-of-kin admitted to SNUBH during the 3-month period from December 2, 2011 to February 13, 2012 in which VDI system was used during physician rounds. Thirty-five participants were selected from each of 7 specialties (pediatrics neurology, pediatrics pulmonology, cardiology, neurology, otorhinolaryngology, rehabilitation medicine, and urology). Eligibility criteria for the survey were: age over 20 years, inpatients or their next-of-kin who can express their opinions without evidence of delirium, confusion or clouded consciousness and had radiology exams during their hospitalization period.
Seven physicians from 7 specialties participated in the survey.
This study was approved by SNUBH's institutional review board (IRB).
5. Survey and Analysis
In the survey, physicians used a mobile environment in which VDI system was accessed through an iPad. The physicians accessed hospital information system while making their rounds through the wards and also used the iPad to directly show patients their progress and results. After these rounds, the physicians who had used the VDI were interviewed about the usefulness of its use, and the patients were also surveyed with a questionnaire.
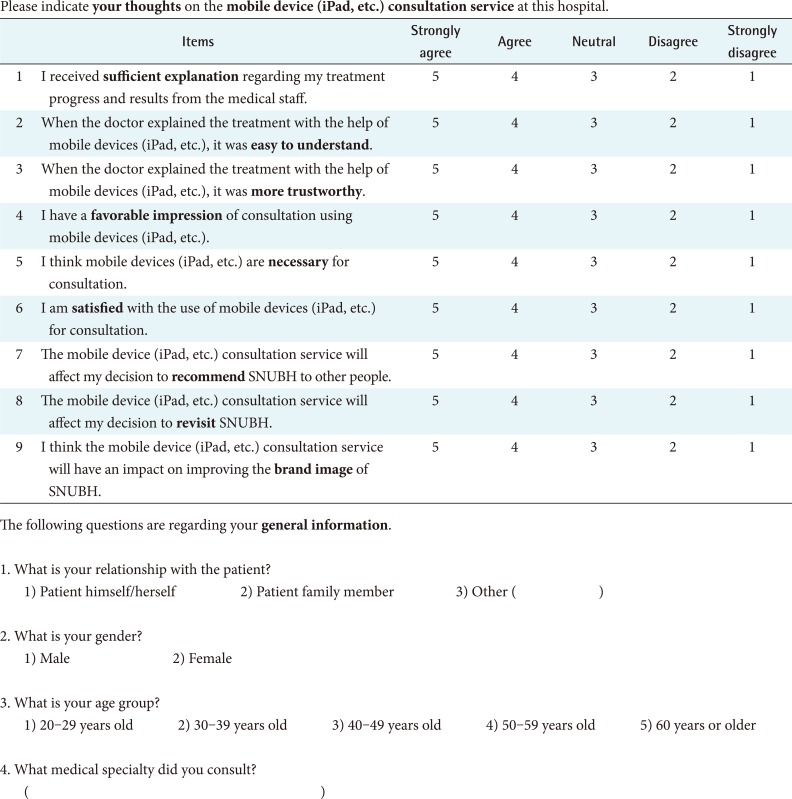
The survey used in this study was composed by a researcher after a literature review, and it consisted of 9 questions in total [17-21]. Of these questions, 6 concerned patient satisfaction, and the remaining 3 questions concerned the revisit, recommendation, and brand image factors (see Appendix A for the questionnaire items in detail). The patient satisfaction consists of the following variables: sufficiency of explanation, ease to understand, trustworthy, impression, necessity, and satisfaction. By performing factor analysis on the six variables, a single patient satisfaction factor was extracted and measured on the average of the variables.
The survey results, measured on a 5-point Likert scale, were statistically analyzed using SAS ver. 9.2 (SAS Inc., Cary, NC, USA).
III. Results
1. Implementation Issues in Establishing VDI-Based Mobile Hospital Environment
During the implementation of the mobile hospital environment using VDI, several concerns arose regarding the design of fault-tolerant system architecture, the privacy and security of patient healthcare information, a mobile device management, the speed and seamlessness of the internal wireless network, the support of screen resolution of legacy clinical applications on tablet PCs, and user education. The followings described the major issues that were derived and resolved in more detail.
Regarding the design of fault-tolerant system architecture, high system availability and stability should be considered to enable the organization-wide adoption of the VDI system. The clustering architecture and dual implementation of servers were considered in our system.
Regarding the privacy and security for the protection of patient healthcare information, secure communication methods and institutional privacy policies should be developed. Technically, the system security was reinforced by employing transmission protocols such as PC-over-Internet protocol (PCoIP) and AD based authorization. We classified end-user groups into private and public users and restricted unauthorized user access to the VDI system with AD-based authorization technique. Demands for the use of the VDI system outside the hospital were issued and supported by allowing access through the VPN and the firewall. The authority was granted only to healthcare faculty in our hospital.
In addition, security concerns created mobile device management challenges. For efficient management, it was necessary to adopt a mobile device management (MDM) system that gave IT staff the ability to view and control all mobile devices.
The speed and seamlessness of the internal wireless network were frequently cited as requirements by the end users who accessed the VDI system using their mobile devices. Thus, the internal wireless network infrastructure should be thoroughly tested before launching a VDI system. Additionally, as the use of the VDI system grew more frequent, it was necessary to expand the access circuit to maintain the network speed.
Regarding the support of screen resolution of legacy clinical applications on tablet PC, during our implementation process, the initial VDI client program did not support the 1,024 ├Ś 768 resolution of our clinical application on the iPad and Galaxy Tab. Verification problems were discovered and resolved before launching the system. Finally, education was necessary for users to become familiar with the user interface of VDI client application, especially when using the system with iPad or Galaxy Tab. Efficient education methods and materials are likely to be a key success factor in system adoption. We utilized online and offline educational methods such as video materials and offline courses.
2. Patient Satisfaction Results
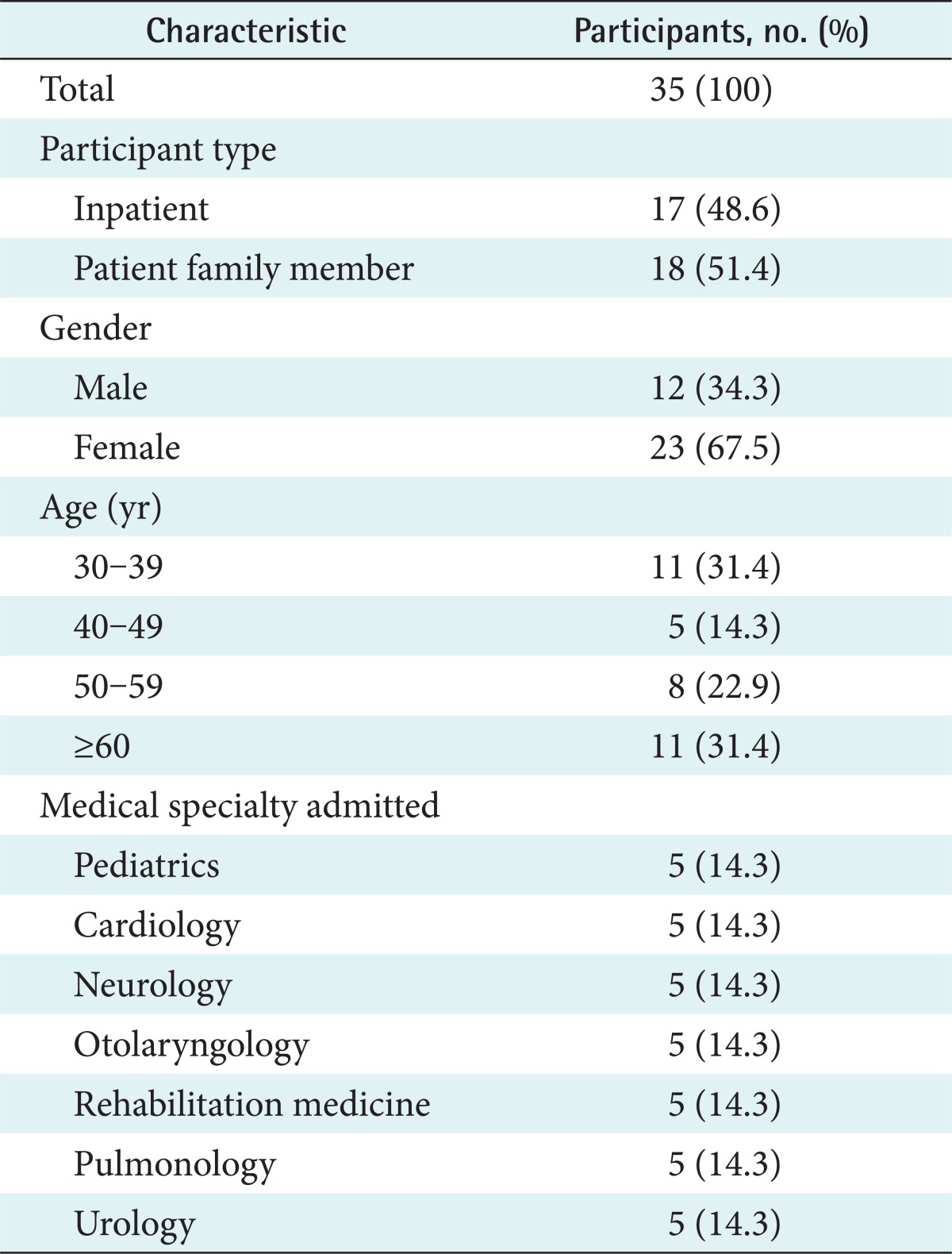
Seventeen patients and 18 patients' next-of-kin participated in the survey. Twelve (34.3%) survey participants were men and 23 (65.7%) were women. Eleven (31.4%) participants were aged 30-39 years, 5 (14.3%) were 40-49 years old, 8 (22.9%) were 50-59 years old, and 11 (31.4%) were 60 years or older. The participants were from the departments of pediatrics, cardiology, neurology, otolaryngology, rehabilitation medicine, pulmonology, and urology. Table 1 shows the general demographic characters of the participants.
Six questions about sufficiency of explanation, easy to understand, trustworthy, necessity, and satisfaction to mobile consultation service were classified as a single averaged variable labeled Patient Satisfaction by factor analysis (Cronbach's alpha, 0.8448).
Table 2 shows the results of the survey, which displayed a "satisfied-level" degree of satisfaction, with average scores over 4 points across all categories. Analysis showed that patient satisfaction did not differ by gender, age, or specialty. A statistically significant difference in patient satisfaction was found between respondents of patients (mean, 4.2) and their next-of-kin (mean, 4.5; p = 0.0369).
Table 3 shows the results of a cross tabulation between patient satisfaction and the 3 influence variables. The results were statistically significant for all 3 items of influence at a level of significance of p < 0.05. The results revealed a significant positive relationship with the patients' decisions on revisiting the hospital and whether the use of VDI improved the brand image of the hospital (p < 0.05).
3. Physician Interview Results
According to the interviews with the 7 physicians who provided the mobile consultation service, the physicians found it useful to be able to explain the patient's progress and results while presenting visual information and, in particular, to be able to instantly check the patient's charts and answer the patient's questions.
However, the degree of physician's satisfaction with the VDI system seemed to differ greatly depending on the user's proficiency with the VDI applications and with iPad operation. In fact, some physicians expressed difficulties in using VDI applications with an iPad, for examples, double-clicking (for 3 physicians), setting up the network (for 4 physicians), and using the automatic screen rotation/hold functions (for 3 physicians). Additionally, concerns arose about the insufficient battery life of iPad and potential extended time of consultation.
IV. Discussion
With regard to VDI implementation at a medical facility, there have been case studies of the successful implementation of desktop virtualization solutions [22,23], but there have been no reports on the application of VDI to real-life consultations or on the issues occurring during its implementation. This study is the first case study report on implementation issues on a mobile hospital environment that utilized full EMR system in VDI system accessed through an iPad. Similarly, security issues implementing a mobile EMR system [24], such as VPN and MDN, were also raised during the implementation of VDI system.
Previous studies reported that VDI enabled unrestricted access to data and information and produced many beneficial effects, including ease in management and cost reduction [6,25]. Additionally, this study showed above the "satisfied-level" of patient satisfaction with the mobile consultation services that utilized VDI and iPad during rounds; interestingly, it also showed that improving patient satisfaction can affect the patients' decisions on revisiting the hospital and a more favorable impression of the hospital.
The limitation of this study would be that the patient satisfaction survey was conducted on only 1 series of inpatient consultation rounds. A study of diverse cases of mobile medical services will need to be conducted in which their impacts are quantitatively evaluated. In addition, this study did not show the evidence that the VDI-based mobile consultation service could improve patient's satisfaction more than other factors such as staff 's kindness, facilities, and expertise. There would be needed a further study to find out what factors would affect more on the patient's satisfaction.
In conclusion, mobile hospital environments have the potential to benefit both physicians and patients. This is the first study that utilized VDI and tablet PCs to implement a mobile hospital environment. From our case study of SNUBH, we found several implementation consideration issues and positive impacts of inpatient satisfaction to the mobile consultation service on hospital's revisit and brand image of the hospital.