I. Introduction
In recent years, cellphones have become an integral part of modern life, and mobile health (mHealth) apps have found their place in the healthcare system [1]. Nonetheless, the success of mHealth technology as a tool to improve healthcare service delivery processes depends on its adoption by healthcare providers [2,3].
Increasing efficiency, reducing costs, and providing healthcare in the least time with the minimum risk are the most important benefits of mHealth [4]. Furthermore, mHealth platforms include multiple functionalities such as education for patients and healthcare providers, diagnostic support, operative planning, postoperative care, and follow-up management [5ŌĆō7].
With the increasing use of smartphones and the growing number of healthcare applications in multiple domains, mHealth is expected to encompass tools that will play an important role in healthcare professionalsŌĆÖ decision-making [8,9]. Nevertheless, it appears that some mHealth applications remain underused by healthcare professionals [10].
Most healthcare providers, particularly physicians, resist using electronic health technologies such as Electronic Health Records, patient portals, online health information, telemedicine, and mHealth [2]. Implementation of these technologies, especially mHealth, implies changes in organizational structures and processes, which often encounter various forms of resistance [11]. Resistance to change is an important barrier hindering the use of new technologies by healthcare providers [12]. Some common barriers include technical, individual, and organizational factors.
Although barriers associated with mHealth adoption in healthcare settings have been addressed in the literature, few studies have systematically reviewed factors influencing the adoption of mHealth. Therefore, there is no consensus on the categorization of barriers to mHealth adoption. Two studies have highlighted barriers and facilitators regarding patientsŌĆÖ and the publicŌĆÖs ability to engage with and use digital health interventions such as telehealth systems, mHealth applications, patient portals, and personal health records [13,14]. To the authorsŌĆÖ knowledge, only one systematic review has been conducted on factors that could facilitate or limit healthcare providersŌĆÖ utilization of mHealth in their work [2]. In that review, the analyzed data were retrieved from four databases between 2000 and 2014. Our study builds upon that previous work, with the aim of conducting a systematic review of more recent literature on barriers associated with mHealth reported by healthcare professionals and identifying the most important barriers.
II. Methods
1. Search Strategy
We adhered to the Preferred Reporting Items in Systematic Reviews and Meta-Analyses (PRISMA) protocol. We conducted a systematic literature search of four electronic databases (PubMed/MEDLINE, Web of Science, Embase, and Google Scholar) to identify studies published between January 2015 and December 2019. We also searched the references of the included publications to identify additional relevant studies. We followed the PICO (population, intervention, comparison, and outcomes) model as a search strategy tool that improves literature searches: (1) the population consisted of healthcare providers (e.g., professionals, physicians, practitioners, providers, residents, clinicians, nurses, midwives, health workers, specialists, dentists, pharmacists, dieticians, physiotherapists, cardiologists, surgeons, gynecologists, ophthalmologists, psychiatrists, and opticians); (2) the intervention was mHealth technology; (3) the comparison was the absence of mHealth technology; and (4) the outcome was reported barriers to adoption of mHealth technology by healthcare providers.
Therefore, the search query included three categories of keywords and their synonyms: barriers, adoption, and mHealth, the definitions of which are presented below.
First, mHealth is a subset of electronic health and refers to the use of portable wireless devices capable of transmitting, storing, processing, and retrieving real-time and non-real-time data between patients and healthcare providers [6,15]. Technology adoption refers to the acceptance, integration, and use of new technology in society and focuses on how a technologyŌĆÖs attributes affect an individualŌĆÖs perception of that technology [16]. Barriers are rules, problems, and similar structures that prevent people from doing something, or limit what they can do [6]. Papers containing these keywords in the title or abstract were searched. The search terms and search strategy are described in Table 1.
2. Study Selection
First, duplicate citations across databases were identified and excluded using EndNote X7.8 (Thomson Reuters, Toronto, Canada) and a manual revision was done for verification. If a study was reported in more than one publication and presented the same data, we only included the most recent publication. In the next step, articlesŌĆÖ abstracts and titles were reviewed according to the inclusion and exclusion criteria. Screening of titles and abstracts was independently conducted by two medical informatics researchers, both of whom are fully versed in mHealth and healthcare systems due to their expertise. The full texts of articles identified as relevant to the objectives were reviewed by the same two researchers. Any disagreement between the researchers was resolved by discussion.
3. Inclusion Criteria
We included articles in this review if they: (1) were full-text journal articles (we excluded abstracts); (2) were published in English; (3) were published in a recent 5-year period (2015ŌĆō2019); (4) reported barriers to mHealth adoption by healthcare providers.
4. Exclusion Criteria
We excluded articles from this review if they: (1) were reviews or gray literature (e.g., conference papers); (2) did not mention the use of mHealth technology; (3) reported mHealth adoptionŌĆÖ barriers from patientsŌĆÖ perspectives; (4) did not address barriers to using mHealth technology.
5. Data Extraction
To extract data and ensure the validity of gathered information, two authors (SZ and TB) extracted barriers to mHealth adoption from all included studies. The corresponding author (AY) then checked the accuracy of the extracted data. In case of any discrepancies, meetings were held to compare our findings and resolve disagreements by discussion.
A focus group discussion was then held with the participation of all authors. Based on the nature of the identified barriers and the opinions of the experts participating in the meeting, the barriers were grouped into three main categories (technical, individual, and healthcare system). Next, each of the identified barriers was assigned to one of the three major categories based on participantsŌĆÖ knowledge and experiences. In this study, due to the nature of the data extracted from the included studies, there was no need for a quality assessment.
III. Results
1. Included Studies
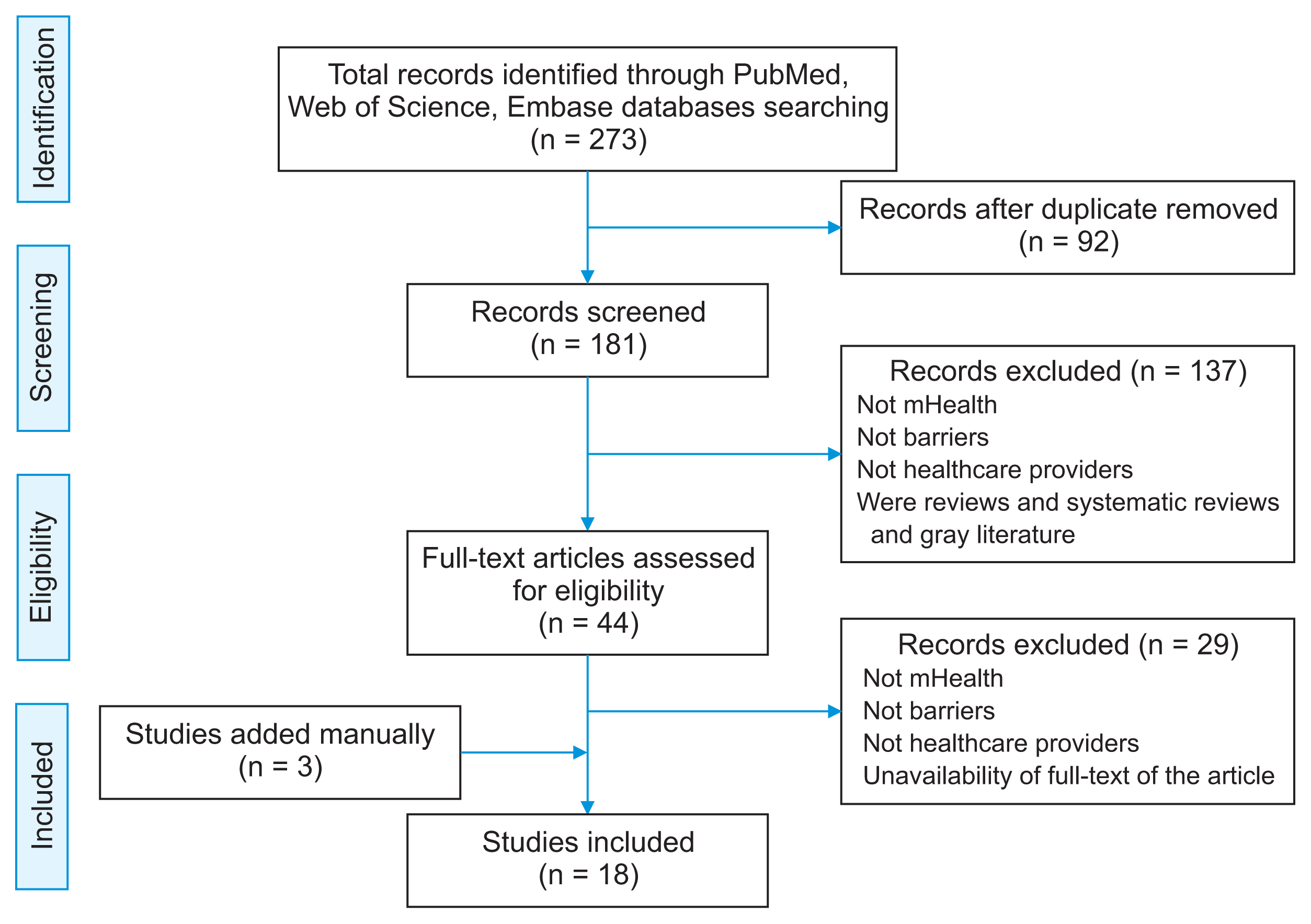
In total, 273 articles were retrieved using the search strategy. Ninety-two duplicates were excluded. After removing the duplicates, the abstracts and titles of 181 articles were studied with respect to the inclusion criteria. At this stage, 137 articles were excluded due to irrelevance of the article title or abstract. The full-texts of 44 articles, which were identified as relevant to the objectives, were investigated. Eighteen articles considered to be eligible were finally included. Three of these articles were found from Google Scholar. Finally, considering the duplication of barriers in different articles, 167 barriers were extracted from the 18 selected articles. The results of the literature search are shown in Figure 1, and the details of each article are summarized in Table 2 [1,17ŌĆō33].
2. Categorization of Barriers
The relevant barriers were categorized into three main groups: technical, individual, and healthcare system. The major categories of barriers to mHealth adoption by healthcare providers are summarized in Figure 2. Technical barriers included eight factors: the lack of existing technology, concerns about regulation and efficacy of applications, security and privacy concerns, user-friendliness, compatibility with the workflow, connectivity speed, a lack of interoperability, and integration with other systems. Individual barriers included five factors: a lack of physician support, resistance to change, difficulty understanding the technology, human appeal, and knowledge and limited literacy. Healthcare system barriers included five factors: legal barriers, reimbursement and accountable care organizations, economic and financial factors, lack of health system policies, and lack of standards.
1) Technical barriers
(1) Lack of existing technology
Healthcare providers, especially physicians, have mentioned a lack of existing technology as one of the largest barriers to greater use of mHealth [17,19]. Technology refers to the collection of techniques, skills, methods, evidence, and processes put into practical use to solve problems [34]. Despite widespread technological advances, there is currently a lack of sufficient evidence-based and specific processes that support the adoption of new technologies, especially mHealth [35].
(3) Security and privacy concerns
In most cases, some aspects are not taken into consideration when developing and releasing a new technology or application. One of the most important considerations is privacy and security, especially in apps that deal with patientsŌĆÖ data regarding their personal and health status, such as Electronic Health Records [25,29,36,37].
(4) User-friendliness
Mobile health platforms offer significant opportunities to improve physician-patient communication and patientsŌĆÖ self-care if they are sufficiently usable [4,38]. These apps have become an essential part of the healthcare field. Their user-friendliness is an essential factor for healthcare providersŌĆÖ satisfaction. The majority of reports on mHealth apps illustrate that a lack of user-friendliness can lead to failure [18,39].
(7) Lack of interoperability and integration with other systems
Interoperability refers to the ability of information systems, devices, and applications to access, exchange, and integrate health data between more than one organization and/or setting of care. A lack of interoperability is often cited as a barrier by healthcare providers because of the burden of their work processes and healthcare costs [18,23,40,41].
2) Individual barriers
(1) Lack of physician support
According to the report released by the World Health Organization (WHO), the use of mHealth technology has changed the image of healthcare delivery worldwide [42]. However, the development of mHealth in the healthcare industry has received little attention from physicians, although healthcare providersŌĆÖ familiarity with and adoption of mHealth technology have a positive impact on its expansion and success [17,21,29].
(4) Human appeal
Mobile technology is changing the way people interact with each other. mHealth technology is used to improve the effectiveness of communication between healthcare providers and their patients [18]. However, the lack of face-to-face human interactions in mHealth technology is a major obstacle to its adoption [17,23,39].
3) Healthcare system barriers
(1) Legal barriers
Legal issues are closely related to the trust issues of healthcare providers. In most countries, because of a lack of legislation, physicians do not trust mHealth applications, and therefore do not accept and work with them. Sands [43] discussed health data sharing and dissemination via mobile devices as physiciansŌĆÖ main concerns due to the lack of corresponding legislation [11,17,18,23].
(2) Reimbursement and accountable care organizations
Reimbursement is another concern of healthcare providers when using new technologies such as mHealth applications for care delivered through these devices. Appropriate reimbursement would require some changes to rules and workflows to overcome some of the current barriers and limitations [17,18,40,41].
(3) Economic and financial factors
These factors refer to the financial resources needed to expand mHealth in rural areas in developing countries. The provision of the tools, equipment, and technological infrastructure to prepare and use these new technologies is not possible without funding resources and economic support [17,19,20,22].
(5) Lack of standards
A standard is an agreed-upon way of doing something, and standards are a key factor for achieving interoperability of healthcare systems and technologies. In addition, healthcare providers believe that a lack of standards, such as identifier standards, messaging standards, structure and content standards, clinical terminology and classification standards, and security and access control standards, hinder the development of mHealth technology. Therefore, technological standards for mHealth need to be developed [4,21,24,28,29].
IV. Discussion
In this review, we identified the literature on common barriers that could limit health professionalsŌĆÖ use of mHealth in their work. Healthcare providers, like many other people, may have a mobile phone or other handheld devices, but this fact does not necessarily mean that they use mobile phones for work purposes. However, given the global focus on mHealth technology, it is important to recognize the factors that affect mHealth adoption by healthcare providers.
The main findings of this systematic review highlight that the identified barriers to mHealth adoption could be classified into three main categories or levels: technical, individual, and healthcare system. Individual-level barriers are directed towards clinicians, physicians, and healthcare providers [44]. Technical-level barriers focus more on network, hardware, and software applications related to the mobile technology devices that clinicians, physicians, and healthcare providers use in the healthcare system [17]. Healthcare system-level barriers refer to managerial attitudes in the system, as well as healthcare policy, standards, and aspects of the financial and reimbursement system [45]. Security and privacy concerns at the technical level, knowledge and limited literacy at the individual level, and economic and financial factors at the healthcare system level were chosen as three of the most important barriers related to the adoption of mHealth in the included publications.
The results of this study are in line with those of the WHO report in 2011, which revealed that security, cost, interoperability, scalability, and lack of local knowledge were the top barriers to mHealth implementation and use. The WHO emphasized that these barriers must be removed before mHealth projects are expanded beyond the pilot stages [26].
The present findings are consistent with those of the systematic review conducted by Gagnon et al. [2], who found that several factors were associated with mHealth adoption at the individual, organizational, and contextual levels. The most important factors identified were privacy and security issues, usefulness and ease of use, time, cost, knowledge of mHealth technology, interactions between healthcare providers and patients, design, and technical concerns.
Our findings also align with those of Laxman et al. [17], who demonstrated mHealth barriers and categorized them as belonging to two levels (system and individual). User-friendliness and a lack of physician support were identified as individual-level barriers, while system-level barriers included security, difficulty understanding the technology, concerns about the regulation and efficacy of applications, human appeal, lack of financial support, and connectivity.
Security and privacy concerns are a major challenge to mHealth adoption [18]. Although mobile technology has revolutionized the way we access information at any time and any place in our lives, consumers of this informationŌĆöand especially healthcare providersŌĆöare concerned about the privacy and security of health-related information. Therefore, healthcare system managers and policymakers must develop appropriate programs, approaches, and policies to ensure privacy and security [46].
The adoption of mHealth offers many benefits to healthcare providers, patients, and managers, as well as other stakeholders. From these healthcare consumersŌĆÖ perspectives, mHealth facilitates access to high-quality healthcare service, communication between patients and clinicians, and collaboration between physicians [47]. Higher-quality and more rapid care can be provided because healthcare providers can access consumersŌĆÖ health information whenever they need it. However, many perceived factors and barriers have hampered the widespread adoption and implementation of mHealth [48]. It will be a time-consuming and challenging process for healthcare providers to overcome these barriers [11].
A major strength of our study is its unique search approach. In the search strategy, we combined elements of qualitative and quantitative research approaches (e.g., the use of qualitative and quantitative viewpoints, data collection, analysis, and inference techniques) to achieve the goals of breadth and depth of understanding and corroboration, and we then used the findings of the identified studies in an integrative manner in our synthesis. Finally, we presented a new classification of barriers related to mHealth adoption by healthcare providers.
Our study has two main limitations. First, we concentrated only on mHealth adoption by healthcare professionals in this review, although it is also important to consider the adoption of mHealth technology in the healthcare system from the perspective of other stakeholders, such as patients and their companions. As Menachemi has pointed out, the opposition and resistance of each of these stakeholders can slow the process adoption [49]. Another limitation of this study is that we did not propose and evaluate facilitators that would increase the adoption of mHealth technology. It is possible that identifying and using facilitators may help overcome the barriers to adopting mHealth technology. This article can be a starting point for future research aiming to identify and evaluate barriers and facilitators of mHealth from the perspective of other health stakeholders.
In conclusion, mHealth adoption is a complex and multidimensional process that is widely implemented to increase access to healthcare services. However, it is influenced by a variety of factors and barriers at the individual, technical, and healthcare system levels. Based on the barriers to adoption identified in this review, security and privacy concerns, knowledge and limited literacy, and economic and financial factors were identified as the top barriers related to the adoption of mHealth. While some authors have focused on the barriers of other information and communication technologies, this systematic review empowered us to identify factors that are specific to mHealth. Understanding barriers to adoption of mHealth applications among providers and engaging them in the adoption process will also be important for the successful implementation of these applications. Therefore, new mHealth applications should focus on these factors in order to facilitate the adoption of mHealth tools to support patient care and to improve their outcomes.