Factors Associated with Website Operation among Small Hospitals and Medical and Dental Clinics in Korea
Article information

Abstract
Objectives
The objective of this study was to investigate the factors associated with website operation among medical facilities.
Methods
A cross-sectional study design was employed to investigate 1,519 hospitals, 33,043 medical clinics (MCs), and 18,240 dental clinics (DCs) as of 2020. The main outcome variable was analyzed according to technological, organizational, and environmental factors.
Results
The percentages of small hospitals, MCs, and DCs with websites were 26.4%, 9.0%, and 6.6%, respectively. For small hospitals, the nearby presence of a subway station (odds ratio [OR] = 2.772; 95% confidence interval [CI], 1.973–3.892; p < 0.0001) was the only factor significantly associated with website operation status. Among medical and dental clinics, the percentage of specialists—MCs (OR = 1.002; 95% CI, 1.000–1.004; p = 0.0175) and DCs (OR = 1.002; 95% CI, 1.001–1.004; p = 0.0061), the nearby presence of a subway station—MCs (OR = 2.954; 95% CI, 2.613–3.339; p < 0.0001) and DCs (OR = 3.444; 95% CI, 2.945–4.028; p < 0.0001), and the number of clinics in the local area—MCs (OR = 1.029; 95% CI, 1.026–1.031; p < 0.0001) and DCs (OR = 1.080; 95% CI, 1.066–1.093; p < 0.0001)—were significantly associated with website operation.
Conclusions
Clinics are critically affected by internal and external factors regarding website operation relative to small hospitals. Healthcare policymakers involved with information technologies may need to pay attention to those factors associated with website dispersion among small clinics.
I. Introduction
Healthcare systems, services, and infrastructure associated with healthcare delivery processes are becoming increasingly digitalized in this era of digital transformation [1]. Digital technologies, such as the Internet of Things and artificial intelligence, are permeating every aspect of healthcare and delivering value to customers [2]. For example, mobile-based personal health record systems allow patients to check the dates of upcoming visits or tests such as computed tomography (CT) or magnetic resonance imaging (MRI) [3,4].
Hospitals and clinics can use websites to educate patients and the public [5], communicate with patients [6,7], and collect patient information [8]. Although some concerns exist about website quality [9,10], websites continue to be indispensable tools in the pipeline of critical healthcare information [11]. According to the American Community Survey, approximately 90% of households had a computer in 2016 [12]. A study found that 68.1% of patients with diabetes accessed personal health records via computers or mobile devices in 2016 [13]. Healthcare providers and healthcare insurance systems present patients with additional opportunities for digital experiences via online access to their medical records [14].
Key topics of study regarding websites include quality, such as that of the information provided overall [15] and for specific areas such as gynecology, infertility healthcare [16], and cancer care [17]. However, few studies have been conducted to analyze the operation or adoption of websites, specifically among hospitals and clinics, using quantitative empirical field data. A study conducted in Italy evaluated the websites of hospitals [18], while researchers in a separate study analyzed the websites of governmental local health departments in Taiwan [19].
Although many people visit the websites of healthcare facilities, a large digitalization gap exists between large hospitals and small clinics, such as medical and dental clinics. Most large hospitals have their own websites, while small hospitals and clinics rarely do. This raises a research question regarding differences between small hospitals and clinics with and without websites. In this study, we investigated this research question based on the technology-organization-environment (TOE) framework of organizational technology adoption following a previous study [20]. While that study was focused on social media adoption, we chose this model because website adoption and social media adoption are similar in promoting consumer engagement [21,22], and both relate to information technology.
The objective of this study was to investigate the factors influencing website adoption by small hospitals and clinics. It is important to understand how many small hospitals have websites and how website adoption differs by type of medical institution.
II. Methods
1. Study Setting
Korea has adopted a national health insurance program wherein the price of a covered healthcare service is uniform within a given type of medical facility, such as hospitals or clinics. For example, the price of an appendectomy is the same across hospitals or clinics. Moreover, patients are free to choose any medical provider [23]. Because the system includes no enrollment or agreement process, they are not restricted to particular providers. Therefore, many healthcare providers are very competitive as they vie for potential customers; ensuring high quality is very important for these institutions because patients can choose providers based on their experience or impression of the quality of care [24]. Consequently, medical providers tend to try their best to keep patients within their system and to maximize their profits in the competitive environment [25]. Websites are useful tools to present various providers’ information to patients and potential customers to aid in their decision-making for better quality of care.
2. Study Design
This study incorporated a cross-sectional design. The units of analysis were small hospitals, medical clinics, and dental clinics, with a total study population of 1,498 small hospitals, 33,366 medical clinics, and 18,345 dental clinics as of 2020. After excluding the units with missing values (3.5% of small hospitals, 1% of clinics, and 0.6% of dental clinics), the final sample comprised 1,445 small hospitals, 33,043 medical clinics, and 18,240 dental clinics. We identified the operation status of the websites of all included institutions in 2020 and explored the characteristics of each category of medical providers regarding website presence. Ethical approval for this study was obtained from the Institutional Review Board of Gil Medical Center (No. GCIRB2021-218) on June 19, 2021.
3. Data Collection
This study incorporated a health insurance administrative dataset that is publicly available from the Health Insurance Review and Assessment Service (HIRA). We collected publicly available data and checked data accuracy between July 1 and August 31, 2021. HIRA’s public domain website, the Healthcare Big Data Hub (https://opendata.hira.or.kr/home.do), provides various types of research data. The HIRA healthcare facility dataset contains information on URLs or website addresses. This information was originally collected as follows: when the founder of a healthcare institution such as small hospitals and clinics reports its establishment as a new facility to the government (local public health department), HIRA collects a report card including URL information and then uses that information for their administrative works.
4. Outcome and Predictor Variables
The outcome variable of this study was the website operation status of the included medical providers. HIRA has collected this information from every medical institution and publicized it through the Healthcare Big Data Hub. The healthcare facility dataset contains information on URL status as of March 31, June 30, September 30, and December 31. In this study, we identified whether each unit had its website URL recorded at all four time points. Specifically, we verified the functionality of each URL using an R program. The institutions with functional URLs were considered to have websites.
The independent variables of this study were also publicly available from HIRA. The different types of medical providers have different characteristics. Thus, in this study, we selected common variables in line with the TOE framework, with the exception of hospital emergency departments (EDs). In general, medical and dental clinics do not have EDs. Thus, this variable was excluded from the main analysis of medical and dental clinics. Regarding market competition, we calculated the Herfindahl-Hirschman Index using the number of beds of each hospital and the residential districts. However, for medical and dental clinics, we used the number of clinics within the same local administrative district as the market competition measure because these facilities generally do not have beds. For the measure of medical and dental specialists, we calculated the proportion of specialists for each medical institution and used it in the final model.
5. Data Analysis
Cross-tabulations were performed and descriptive statistics were analyzed based on the website operation status (yes or no). To compare the frequency and mean difference between two groups, we used the chi-square test and t-test, respectively. Before the main analysis, correlations among the independent variables were investigated. No set of variables had a correlation higher than 0.6. For the main analysis, this study employed logistic regression given the binary outcome variable (website presence or absence). Specifically, this study presented three models: small hospitals, medical clinics, and dental clinics. No substantial correlations were observed among the technological, organizational, and environmental factors and the targeted independent variables. Thus, we included all of the general characteristic variables and the target independent variables in each model and presented the adjusted odds ratios. R software version 4.1.1 (R Foundation for Statistical Computing, Vienna, Austria; https://cran.r-project.org/) was used to verify the website URLs provided by HIRA. SAS version 9.4 software (SAS Institute Inc., Cary, NC, USA) was used for statistical analysis.
III. Results
1. General Characteristics of Study Subjects
Table 1 presents the basic characteristics of small hospitals, medical clinics, and dental clinics by their website operation status. The percentages of small hospitals, clinics, and dental clinics with functional websites were 26.4% (381/1,445), 9.0% (2,967/33,043), and 6.6% (1,204/18,240), respectively.

General characteristics of the facilities by website operation status
Among the main independent variables based on the TOE framework, small hospitals with websites were more likely to have CT or MRI capabilities, operating rooms, emergency departments, and nearby subway stations than those without websites (p < 0.05). Medical and dental clinics with websites had a greater likelihood of having CT or MRI scanners, a higher proportion of medical and dental specialists, and nearby subway stations (p < 0.05). While the medical clinics with websites were more likely to have operating rooms (p < 0.005) than the medical clinics without websites, the dental clinics with websites were more likely to be in a competitive environment (p < 0.005) than those that lacked websites.
2. Small Hospitals
Table 2 presents the factors associated with website operation for small hospitals with more than 30 and fewer than 100 beds. Among the TOE factors, only an environmental factor, the presence of a subway station near the hospital (odds ratio [OR] = 2.771; 95% confidence interval [CI], 1.973–3.892; p < 0.0001), was significantly associated with website adoption and operation. Specifically, the odds of having a website were 2.771 times greater among small hospitals with nearby subway stations than among those without subway stations. Of the general characteristics, years of operation (OR = 1.081; 95% CI, 1.064–1.098; p < 0.0001) and the number of physicians (OR = 1.025; 95% CI, 1.002–1.048; p = 0.030) were significantly related to website adoption (p < 0.05).

Factors associated with website operation among small hospitals
3. Medical Clinics
Table 3 shows the factors associated with website operation for medical clinics. Among the TOE factors, both organizational and environmental features were associated with website adoption. The percentage of specialists (OR = 1.002; 95% CI, 1.000–1.004; p = 0.0175), the presence of operating rooms (OR = 2.400; 95% CI, 2.139–2.691; p < 0.0001), the nearby presence of a subway station (OR = 2.954; 95% CI, 2.613–3.339; p < 0.0001), and the number of medical clinics in the local area (OR = 1.029; 95% CI, 1.026–1.031; p < 0.0001) were significantly associated with functional website status.
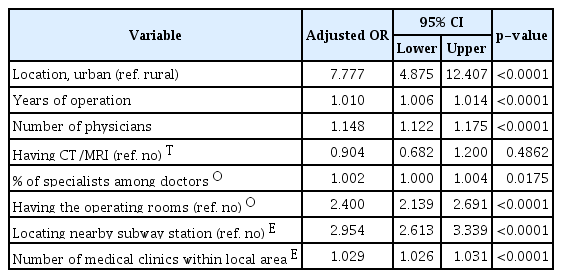
Factors associated with website operation among medical clinics
4. Dental Clinics
Table 4 presents the factors associated with website operation for dental clinics. All TOE factors were associated with website operation status except the presence of operating rooms. CT or MRI capabilities (OR = 1.323; 95% CI, 1.140–1.534; p = 0.0002), the percentage of specialists (OR = 1.002; 95% CI, 1.001–1.004; p = 0.0061), the nearby presence of a subway station (OR = 3.444; 95% CI, 2.945–4.028; p < 0.0001), and the number of dental clinics in the local area (OR = 1.080; 95% CI, 1.066–1.093; p < 0.0001) were significantly associated with website operation.

Factors associated with website operation among dental clinics
IV. Discussion
In this study, we investigated the factors associated with website operation among small hospitals, medical clinics, and dental clinics. Based on health insurance administrative data, the rate of website adoption was found to be 26.4% in small hospitals, 9.0% in medical clinics, and 6.6% in dental clinics. For small hospitals, years of operation, the number of physicians, and the nearby presence of a subway station were significantly associated with website operation status. In contrast, the location of the facility, years of operation, number of physicians and dentists, nearby presence of a subway station, and the number of local clinics of the same type were significantly associated with website operation status for both medical and dental clinics. In addition, having a website was significantly associated with having beds, operating rooms, and physical therapy rooms among medical clinics and with the percentage of dental specialists as well as CT and MRI capabilities in dental clinics.
Approximately 27% of small hospitals had websites. According to a study conducted in Taiwan, about 60% of the 417 hospitals studied had web-based appointment systems [7]. A study conducted in Italy in 2010 showed that 60.3% of all hospitals had websites [17]. Assuming that Korea has around 350 general hospitals, including 43 tertiary hospitals, and that all of those hospitals have websites, the estimated proportion of website presence is roughly 40.8% ([350×100+1445×26.4]/[350+1445]), which is much lower than those of Taiwan or Italy, which are the only available comparable figures on website adoption rates. Regarding website adoption among clinics, fewer than 10% had their own websites. No comparable study has been conducted for comparison; however, given that in the United States, many small clinics are affiliated with large health maintenance organizations that offer clinic information, most providers, including hospitals and clinics, may have their own websites. This suggests that the website adoption rate among Korean medical and dental clinics is also much lower than that among providers in the United States.
In this study, the rate of website adoption was much higher among small hospitals than among medical and dental clinics. This makes sense if we consider several perspectives. Constructing and maintaining websites is costly, including both a fixed cost that is not dependent on the size of the medical facility and an operating cost for maintenance. Thus, it would be difficult for small clinics, with correspondingly small profits, to design and manage websites. In contrast, hospitals, with their relatively large revenues, are likely to have websites because their larger revenues are a source of investment for website development.
In addition, small hospitals, medical clinics, and dental clinics located in areas with a high floating population and good transportation may perceive websites as necessary to compete with large, reputable hospitals and clinics to increase advertisement effects and reveal their presence to people passing nearby their location.
This study yielded four interesting findings. First, only a few factors were significantly associated with website operation among small hospitals, while more variables were associated with website operation among medical and dental clinics. A clear difference was observed between small hospitals and clinics. The size of the organization seems to have a differential impact on website adoption. Small size, by itself, indicates a lack of economies of scale [26,27], which may make the facility more sensitive to external and internal factors such as internal operating costs, threats of closure, or mergers [28,29]. Thus, those external factors may critically affect the adoption of websites among clinics. Second, most of the measured variables of medical and dental clinics were associated with website operation in a similar fashion. A possible interpretation of this finding is that although general healthcare and dental healthcare differ in the types of health services provided, they are also broadly similar in facility size and purpose (the provision of healthcare). Thus, the same measures were similarly associated with website operation for both types of facilities. Third, the percentage of website adoption seems to be closely associated with environmental factors such as urban location, transportation infrastructure (such as subway stations), and market competition. If an environment has good infrastructure for healthcare businesses, such as transportation and location, then clinics with websites would realize many benefits in advertising the facilities and revealing information to potential customers. This may explain why environmental factors were associated with website adoption. Fourth, the likelihood of website adoption increases with the size of small hospitals, medical clinics, and dental clinics, as measured by the number of physicians and dentists. This result may be supported by a previous finding in which advertising expenditure increases with hospital size as measured by the number of beds [30]. As the size of hospitals, medical clinics, and dental clinics increases, more features exist to advertise and describe to customers, such as medical staff and the operating status of advanced medical equipment. Thus, economies of scale seem to apply in this case as well.
This study had several limitations. First, although we used several procedures to identify facilities with websites, website presence among this group may still have been underestimated. Small hospitals and clinics may launch websites after their initial reporting to HIRA as not having websites. However, this study incorporated the whole facility population as the unit of analysis, and thus, the underestimation would not have critically affected the results. Second, this study did not include any information on patients, such as the total number of patients, in the model. Given that websites are a good information source, a relationship may exist between website operation status and the number of patients. Third, we directly used the measured variables in absolute instead of relative terms. Although using relative terms could increase the validation of the study results, we were concerned about potential distortion of the measured figures of variables and thus used the original variables in absolute terms. Hopefully, future studies can consider these limitations.
Despite its limitations, this study is important from several perspectives. First, it is the first study to investigate website operation status using empirical quantitative, national-level data. None of the previous studies utilized similar data sources. Second, while every nation has a different healthcare system, countries primarily use national health services or national health insurance systems. As it was conducted within the national health insurance system in a competitive environment, this study could provide insight to other countries about website adoption by small hospitals and clinics under national health insurance systems. Many patients can obtain valuable information or convenience from the websites of medical facilities [2,7,16]. As such, this topic requires further study.
In conclusion, approximately 26% of small hospitals with 30 to 100 beds, 9% of medical clinics, and 7% of dental clinics had their own websites in Korea, revealing a large gap between small hospitals and clinics. Various characteristics of medical and dental clinics were associated with website operation status that were not significant among small hospitals. To ensure better access to healthcare and enhance patient convenience, governments and large insurance companies may need to provide support for clinics to run their websites. Small changes in healthcare systems would bring substantial convenience to patients and their families in this era of digital transformation.
Acknowledgments
We thank Mr. Ji Soo Jeon, Department of Biomedical Engineering, Gil Medical Center, Gachon University, for the assistance conducting the actual verification of HIRA’s website URLs of hospitals with the reported records using the R program. This research was supported by the MSIT (Ministry of Science and ICT), Korea, under the ITRC (Information Technology Research Center) support program (No. IITP-2021-2017-0-01630) supervised by the IITP (Institute for Information & communications Technology Promotion), and by the GRRC program of the Gyeonggi province (No. GRRC-Gachon2020 (B01).
Notes
Conflict of Interest
Kwang Gi Kim is an editorial member of Healthcare Informatics Research; however, he did not involve in the peer reviewer selection, evaluation, and decision process of this article. Otherwise, no potential conflict of interest relevant to this article was reported.