Implementation of Consolidated HIS: Improving Quality and Efficiency of Healthcare
Article information
Abstract
Objectives
Adoption of hospital information systems offers distinctive advantages in healthcare delivery. First, implementation of consolidated hospital information system in Seoul National University Hospital led to significant improvements in quality of healthcare and efficiency of hospital management.
Methods
The hospital information system in Seoul National University Hospital consists of component applications: clinical information systems, clinical research support systems, administrative information systems, management information systems, education support systems, and referral systems that operate to generate utmost performance when delivering healthcare services.
Results
Clinical information systems, which consist of such applications as electronic medical records, picture archiving and communication systems, primarily support clinical activities. Clinical research support system provides valuable resources supporting various aspects of clinical activities, ranging from management of clinical laboratory tests to establishing care-giving procedures.
Conclusions
Seoul National University Hospital strives to move its hospital information system to a whole new level, which enables customized healthcare service and fulfills individual requirements. The current information strategy is being formulated as an initial step of development, promoting the establishment of next-generation hospital information system.
I. Introduction
A hospital information system (HIS) is an information system supporting best practices and efficient hospital administrative activities [1]. Mainly, it is composed of electronic medical records (EMR), picture archiving and communication systems (PACS), computerized physician order entry (CPOE) which is also called order communication systems (OCS) in Korea, and management information systems.
Seoul National University Hospital (SNUH) was established in 1885 as Korea's first national hospital which was the affiliate hospital for Seoul National University's College of Medicine and College of Dentistry, before begin recognized as a special corporate body under the name of Seoul National University Hospital. Today SNUH is comprised of the Main Hospital, the Children's Hospital and the Clinical Research Institute. Over 1,700 hospital beds, approximately 1,600 inpatients and 7,100 outpatients are treated each day by about 500 medical professors and about 4,500 staff.
The emergence of digitalization in clinical environments has played a major role in boosting efficiency and customer satisfaction. SNUH discontinued the use of paper-based clinical order sheets by adopting OCS in 1999. It also moved to filmless environments by adopting PACS in 2001. The third update was the adaptation of EMR in October 2004, through which SNUH completely changed its digitalized environment for clinical activities [2]. Such digitalization facilitated systematic data management, which supported cost savings in data restoration, improvement in data reliability and accessibility, and enhancement of information sharing among clinicians.
Among the general hospitals in Korea, SNUH is the first to implement EMR. Seoul National University Bundang Hospital (SNUBH), which is a sister hospital of SNUH, launched EMR first in 2003. There was less resistance in adopting EMR, as it was a newly opened hospital. With the mission of achieving a fully digitalized hospital, it successfully implemented EMR.
After successful implementation of EMR at SNUBH, SNUH tried to customize SNUBH's EMR system. It took a year for the customization to be completed. Through the customization, various defects and supportive adjustments were defined and amended before the adoption. For the successful customization, SNUH developed up to 3,000 new medical record templates and revised diagnostic terms and procedure terms and the corresponding codes. These were driven by medical record specialists and were mapped to Internaltional Classification of Diseases-10 (ICD-10) for insurance reimbursement.
After five years of successfully implementing EMR, it is currently a popular information system in the healthcare arena, as many general hospitals in Korea run EMR systems successfully. This paper gives a brief description of the information system in SNUH.
II. Case Description
The HIS of SNUH consists of diverse inter-operative systems that perform fundamental activities within the hospital, fulfilling both clinical and managerial perspectives (Figure 1). Each of these systems is composed of a set of interfaces and applications, individually specialized to assist certain features and requirements. The characteristics and architecture of these components in HIS are as follows:
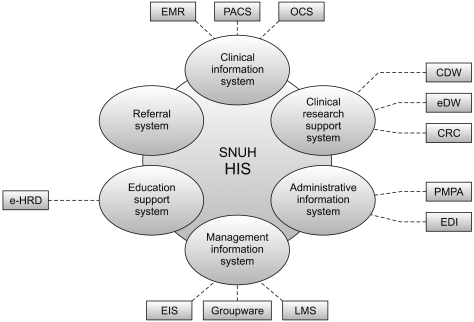
Components in the hospital information system (HIS) of Seoul National University Hospital (SNUH). CDW: clinical data warehouse, eDW: enterprise data warehouse, CRC: clinical research coordinator, e-HRD: electronic human resource development, PMPA: patient management patient accounting, EDI: electronic data interchange, EIS: executive information system, LMS: logistics management systems.
1) Clinical information system
This is designed to support the clinical activities of physicians and nurses. The main components are EMR, PACS, and OCS. EMR is for the records of clinical activities, and OCS is for billing and the administration of patients, which are closely related concepts.
2) Clinical research support system
This can be classified into two groups: a clinical data repository and a system for research-oriented data management. The clinical data repository is an integrated database for statistics. Mainly, it is used for finding and developing various clinical indicators to promote and evaluate clinical and research activities. It includes the clinical data warehouse (CDW) and the enterprise data warehouse (eDW). For research data management, SNUH built a clinical research coordinator (CRC) system.
3) Administrative information system
This is a part of the OCS system related to patient registration, admission, and discharge, called patient management patient accounting (PMPA). In addition to handling patient administration, it has a billing system and an electronic data interchange (EDI) system for insurance reimbursement.
4) Management information system
This is a system that is optimized to support administrative management over organizational resources, including human resources, accounting, inventory and others. This system interacts with a number of internal applications, such as payroll, accounting, human resource management, and logistics management systems (LMS), covering everything from drugs to stationery. In addition, business operational management and communication within the hospital are assisted by an executive information system (EIS) and a groupware, respectively.
5) Education support system
This was developed to stimulate the proficiency and competency of the performances of all employees in the hospital. This activity is supported by a specially designed electronic human resource development (e-HRD) system.
6) Referral system
SNUH provides an official website for users to reserve and confirm online registration. Moreover, a medical data interchanging system encourages a cooperative alliance between medical centers by providing easy-to-use data transaction environments.
III. Results
A detailed description of HIS will be presented as follows, beginning with clinical information system (CIS).
1. CIS
CIS is a system supporting clinical activities, in which EMR and PACS intervene as major applications. As SNUH is the first general hospital that has successfully replaced a conventional care delivery system with a fully digitalized healthcare system, the HIS of SNUH has provided important frameworks of pragmatic medical informatics, including data format, data interchange protocols, and various codes for diagnosis, treatment, and procedures.
SNUH assigns different access levels of CIS based on the role of each practitioner. The access level is classified according to the practitioner's task, profession, and responsibilities. Through the systemic control of the access level, SNUH has enforced stronger awareness of privacy responsibility. This not only controls unauthorized access from outside, but also limits unauthorized access beyond the practitioner's assigned level due to a strong ban by a special privacy protection group.
1) EMR
One of the distinguished advantages of EMR is the use of standard clinical vocabulary. In the early stages of development, which was in 1999 for the development of OCS, a team of physicians was organized to develop medical terminologies for diagnoses and procedures. In the beginning of this work, they collected medical terminologies and analyzed them from the legacy system. After working on harmonization, they built medical terminologies for the digitalized medical records. SNUH incorporated ICD-10 and local codes as standard content to facilitate the maintenance of terminology and to preserve on-going practice. For the future, the use of all the terms will be mapped to systematized nomenclature of medicine-clinical terms (SNOMED-CT).
Another distinguished feature of EMR is the improvement in information sharing between hospitals. SNUH enabled the interchange of EMR across sister hospitals (SNUBH, Boramae Medical Center, SNUH Healthcare System Gangnam Center) by providing a medical record viewer. The sharing of EMR leveled up patients' satisfaction by decreasing the inconvenience of switching hard copies of medical records from one institute to another. The closeting of information slows the provision of health care, endangers lives and makes it exceptionally difficult to track patient outcomes. The environment for information sharing enables physicians to best meet the needs of patients.
The nursing information system of EMR has many advantages that support nursing activities. The most prominent is the nursing statements. In 2004, SNUH made a standard nursing statement and maintained nursing processes. The statement covers the standardization of terminology appropriate for clinical nursing, nursing assessment, nursing estimation, nursing diagnosis, and nursing planning. Recognizing the need for internationalization, the nursing system uses International Classification for Nursing Practice (ICNP) Beta 2 codes.
The nursing note based on post-coordinated statements has improved the quality of nursing records. Instead of using free text, it uses predefined statements. As nursing notes are expressed with predefined unit expressions, we can easily implement a program for nursing notes with a clinical decision support system [3]. In addition, it helps to clarify and analyze nursing activities, which used to be ambiguous and difficult to evaluate. At present, there are 3,769 nursing assessments and estimation statements, 5,524 nursing diagnoses, and 214 nursing plans.
Patient safety is a top priority when considering nursing applications. When EMR finds the same patient name in a nursing unit, it automatically adds an extra letter of the alphabet following the names of patients.
EMR has a strong double-check system for the verification of blood transfusions. To make sure that each data entry is based on accurate content, EMR uses a barcode system for checking the order of the blood transfusion (Figure 2). A barcode on a blood bag is scanned and automatically checks the patients name, sex, age, blood groups, and doctor's order on the screen. These timely and accurate data verifications minimize possible errors and enforce clinical participants' patient safety.
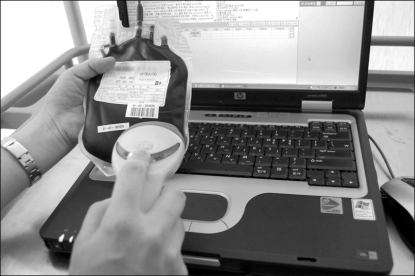
Barcode system for blood transfusion.
2) PACS
Declaring itself to be a filmless digital hospital, SNUH adopted PACS in July 2001. Since then, it has used the PACS effectively for patient care, research, and education. There are many kinds of PACS in SNUH: PACS for still images, video PACS for endoscope video images, PACS for cardiovascular center, radiotherapy PACS, 3D PACS for three-dimensional volume rendering, virtual private network PACS for interpretation of images in case of emergencies outside the hospital, and Web PACS for viewing key specified pictures on the web.
One of distinguished features of PACS is its capacity of holding and handling images. Although the size of the total image database is up to 400 TB, it presents images in a short period of time. As it holds all images from 2001 in the active storage device, all images can be reviewed from PACS without any uploading processes. Additionally, the efficiency of the PACS data management has been significantly improved through access level control. PACS data can be classified into two different types: active and inactive data. PACS classifies the data of patients who are either dead or have not received any clinical treatment for over 5 years as inactive.
In terms of inter-operability, SNUH's PACS is the first in the world to transfer conventional endoscopic video to digital imaging and communications in medicine (DICOM) MPEG-2 images. In addition, SNUH provides a counter acceptance outside PACS images. The establishment of this new process minimized inconvenience for patients and improved efficiency for better healthcare delivery. Furthermore, this progression presented a new model for the data transition of other clinical institutes.
For data protection, PACS has a mirror storage system, which enables a real-time recovery when a systematic failure occurs.
2. Clinical Research Support System
The clinical research support system provides up-to-date, accurate clinical data, used as a resource for various clinical laboratory tests and for the establishment of innovative care-giving procedures. This system can be classified into a clinical data repository and a research data management system. SNUH uses the CDW and eDW as clinical data repositories and has a CRC system for the research data management system.
1) CDW & eDW
Computer-based records have great merit for the comprehensiveness of an overall spectrum of clinical data. Therefore, SNUH founded an overall data warehouse (DW) for data assembly to facilitate data analysis. SNUH manages two DWs: one of which is the CDW and the other is the eDW, which is being prepared for activation in the near future.
The CDW system is a central repository containing the clinical and administrative data of the HIS. It supports various clinical research activities. It also delivers key data for the analysis of clinical performance or management efficiency, which enables users to evaluate a wider range of data analysis, regardless of time or place. It is capable of collecting the required data through an easy-to-use ad-hoc query set by the user without interfering with the speed of the operation of the main DW (Figure 3).
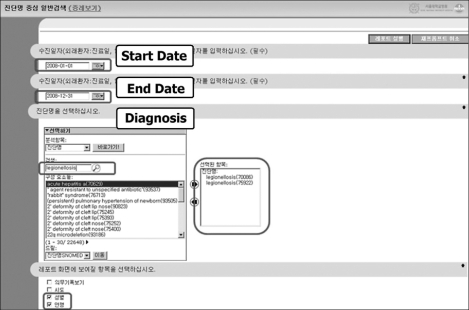
Clinical data warehouse.
As the CDW provides comparative statistics based on selective subjects of the collected data, it provides a comparative statistic of collective data for innovative analytical and research activities through constant monitoring.
A new DW system, named eDW, is under development to improve analysis ability and usability and to expand the coverage of data beyond that of the CDW. Currently, the eDW has been developed for four surgical departments and two internal medicine departments, and the test services were launched in August 2010. In the near future, the coverage of the eDW will be expanded to the entire hospital information system, and the quality of the eDW will be improved.
2) CRC system
SNUH established the CRC system in 2007 in response to the demands of clinical researchers. In the beginning, they requested an independent system for clinical research activity supporting the reported work and data management, but after a long investigation, SNUH decided to provide a specialized system for researchers. The research support system, named CRC, deals with research reporting and describing clinical findings. As there are many types of researchers involved in the same project, the CRC has the function of assigning different access levels of EMR.
Privacy protection is an important issue even in the research domain. Disclosure of confidential information is strictly regulated by the system and by a monitoring group of SNUH. The access of clinical research coordinators is permitted only for designated patients recruited for the study. They are capable of reviewing only the necessary information authorized within the scope of their study.
IV. Discussion
In June 2009, SNUH received ISO 27001 certification, which was the first ever certificate in the medical informatics arena in Korea [4]. ISO 27001 is an information security management system standard published by the International Organization for Standardization (ISO) [5]. This certificate is accredited when the assessments for 11 parts of 133 items, including risk management, information security policy, information security organization, classification and management of information assets, are passed.
Because SNUH emphasized privacy protection above all other activities, achieving the certificate is a very encouraging historical moment. The operation of the whole system without any privacy breach is a difficult task. The level of privacy is only adequate when an organization has a good privacy protection system, powerful regulations, monitoring activities, and education.
SNUH has just begun development for the next-generation HIS. One of the new visions of the next-generation HIS is providing personal health records to the whole population while they are still healthy [6]. Regarding the new vision, patient safety is also an important key element to be solved through the next-generation HIS. The new service name, personal health record (PHR), has many sophisticated requirements. Because there are stricter regulations in health information in Korea compared to other countries, PHR service has not yet been introduced in Korea. However, we envision a new health environment, in which all the medical records are shared easily among hospitals, and all the health data collected from houses are easily shared between doctors and patients.
Another reason for developing the next-generation HIS is to prepare the SNUH medical center. In other words, from an informational point of view, the integrated medical center can be completed by the next-generation HIS. A roadmap of next-generation HIS development has already been constructed, and as the first step, information strategy planning (ISP) for developing the next-generation HIS is currently underway.
For years, SNUH has tested many kinds of u-health devices and has participated in various clinical researches using u-health technologies [7-9]. Providing refined processes for protecting the privacy and security of patient information, we think that the implementation of PHR is in the near future. For the realization of new-generation health informatics, the experience from launching EMR will provide important guidelines for leaping to the new generation of healthcare information.
Acknowledgements
This article was supported by grant number 042 007 0750 from the SNUH research fund.
Notes
No potential conflict of interest relevant to this article was reported.