Design and Realization of Integrated Management System for Data Interoperability between Point-of-Care Testing Equipment and Hospital Information System
Article information
Abstract
Objectives
The purpose of this study was to design an integrated data management system based on the POCT1-A2, LIS2-A, LIS2-A2, and HL7 standard to ensure data interoperability between mobile equipment, such as point-of-care testing equipment and the existing hospital data system, its efficiency was also evaluated.
Methods
The method of this study was intended to design and realize a data management system which would provide a solution for the problems that occur when point-of-care testing equipment is introduced to existing hospital data, after classifying such problems into connectivity, integration, and interoperability. This study also checked if the data management system plays a sufficient role as a bridge between the point-of-care testing equipment and the hospital information system through connection persistence and reliability testing, as well as data integration and interoperability testing.
Results
In comparison with the existing system, the data management system facilitated integration by improving the result receiving time, improving the collection rate, and by enabling the integration of disparate types of data into a single system. And it was found out that we can solve the problems related to connectivity, integration and interoperability through generating the message in standardized types.
Conclusions
It is expected that the proposed data management system, which is designed to improve the integration point-of-care testing equipment with existing systems, will establish a solid foundation on which better medical service may be provided by hospitals by improving the quality of patient service.
I. Introduction
The use of point-of-care testing (POCT) is remarkably increasing [1]. POCT equipment may be used anytime and anywhere, and it enables medical staff to make a quick diagnose and treat patients, contributing to improvement of patient satisfaction by reducing the amount of blood collection. Also, it may improve the efficiency of work carried out by clinicians, who have to take care of many patients in a short time. Due to the various advantages of POCT, the equipment occupies one third of the in vitro diagnostic (IVD) testing equipment markets in the world, and medical service based on POCT equipment is growing by 9% per year [2,3].
However, various problems need to be overcome before the introduction of POCT equipment in a given system to achieve the efficiency mentioned above. Of course, a hospital is a medical service institute where patients are treated, so time-based factors are involved the in treatment of patients. When we consider such factors from the perspective of medical service, it may be compared in terms of therapeutic turnaround time (TTAT) [4]. The TTAT refers to the total period from a clinicians issuance of order, delivery of order, collection of specimen, transportation, pre-treatment, calculation of results, verification, delivery of results, and start of treatment. In this procedure, the POCT plays a role in reducing the time required for the delivery of order, transportation and pre-treatment of specimen, and delivery of results [5,6]. Such functions cannot be covered using POCT equipment; rather, the equipment is used on the premise that it is inter-operable with the existing hospital data system.
Therefore, hospitals are making efforts to solve these problems by installing a server between the POCT equipment and the laboratory/hospital information system, where the POCT data management system (DMS) is constructed. However, in reality, the current hospital data system is optimized to the centralized testing process, and the system is inefficient to integrate heterogeneous data generated by each type of equipment [7].
To ensure interoperability between the POCT equipment and the existing hospital information system, many factors must be taken into account.
First, problems related to connection persistence and reliability may occur when mobile equipment is introduced to an existing hospital data system which is optimized to the centralized testing process. This may cause delay in the delivery of test results, and this can lead to loss of data and omission of insurance claims [8]. Second, the current data systems in hospitals have such inefficient structures that they may not properly integrate disparate data generated by various products and manufacturers. Third, it is still uncertain as to how to deal with problems related to the results without test orders, which occurs due to the characteristics of mobile equipment.
To address these issues, we need to carry out studies aimed at designing more automated and streamlined systems.
II. Case Description
1. System Design
1) System composition
The entire composition is divided roughly into the equipment domain, DMS domain and hospital data system domain.
2) DMS design
The overall details are designed as a total framework according to the POCT1-A2 standards [1].
First of all, the device connectivity management agent (DCMA) and connection management agent (CMA) are positioned to ensure the connection persistence and reliability of each piece of equipment on the basis of the bottom physical interface layer. This defines the details related to the physical and logical connection and communication methods of the equipment. The data generated in the connected equipment is collected comprehensively by the integrated gateway agent (IGA). This is defined as the conversion method in which many types of heterogeneous data are transformed into standardized messages. Lastly, the application service layer provides a service-type function by applying the data stored in the DMS database.
3) Major agent, service design, and movement
(1) DCMA
The existing hospital environment has such vulnerable structure that it cannot ensure connectivity in which the mobility of POCT equipment is reflected. Therefore, we propose a method that can ensure efficiency of maximum connectivity in a TCP/IP environment in which a wire/wireless LAN is universally used. Figure 1 shows the design and actions of the DCMA, which improves of connection persistence in a TCP/IP environment.

Device connectivity management agent.
(2) Design and actions of CMA
To improve the connection reliability among equipment connected to the DMS, a CMA shall play its own role. The operational method of this agent is based on the lower-layer communicational standards provided by the LIS1-A [9].
Basically, after classifying the communicational state into establishment phase, transfer phase and termination phase, the protocols suitable for each state are realized [10,11]. Then, the rules related to error detection, error recovery, time out, message re-transmission count, and interrupt method, which may be applied to each state, are reflected in each state.
Showing the diagram of CMA actions that ensure connection reliability, Figure 2 presents the actions that shall be taken in each state.
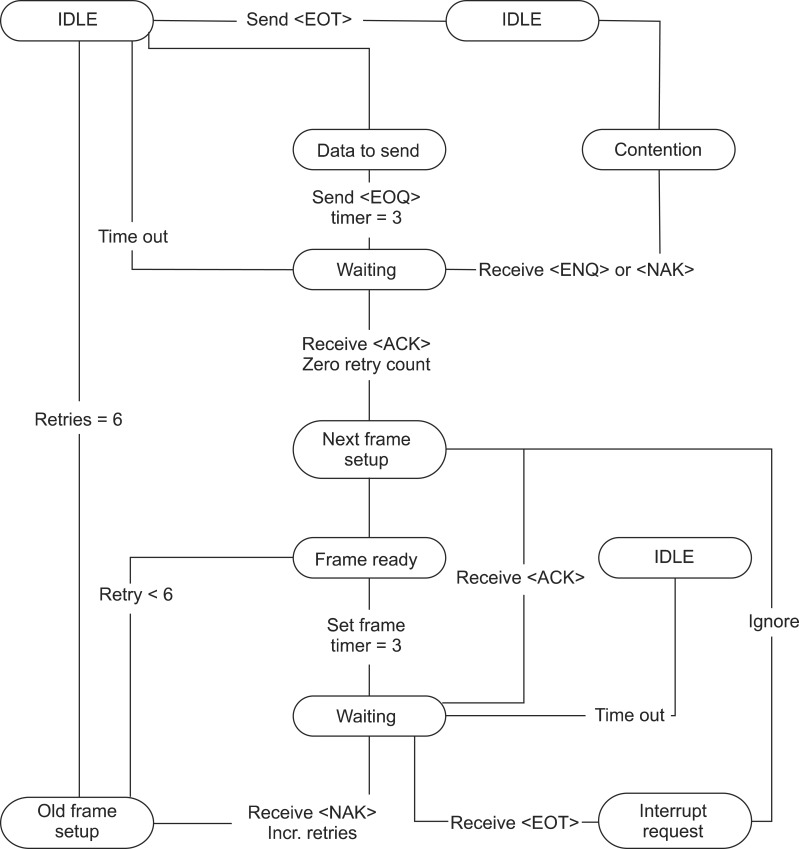
Connection management agent state diagram.
(3) Design and movement of IGA
The types of messages generated in equipment connected by a subagent may not be based on a standard, or a message may not assume a consistent message from due to the difference and ambiguity of field meaning, although the message is based on the standard. Accordingly, it is necessary to reinforce the function that can integrate disparate data into a standardized type of message and deliver the message after converting it into the form required by the hospital information system. Figure 3 shows the design and movement of the ISA that play this role.
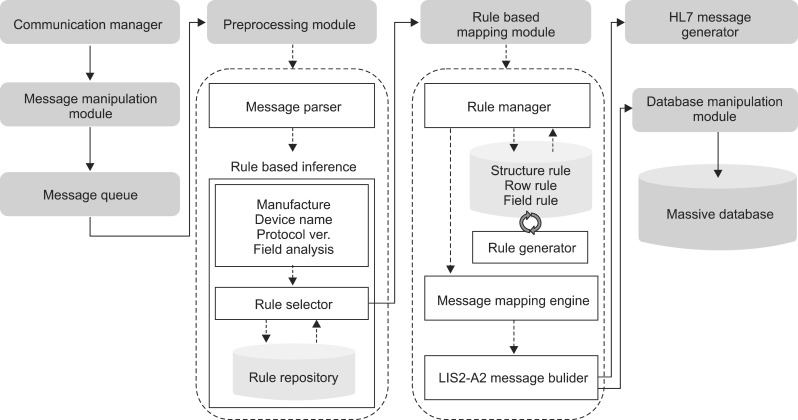
Integration gateway agent structure.
(4) Design and movement of auto order request service
The order generation procedure in a POCT environment is different from that of a centralized testing process. In general, the order request service in a centralized testing processor seems to be a type of pre-ordering and post-testing, in which an order is entered into the hospital information system and the test is carried out after a clinician has placed the order.
However, in a POCT environment, the order request service is carried out in a type of pre-testing and post-ordering, in which the order is placed after testing has been completed. In this type of work procedure, the medical staff is not able to know if an order has been entered into the hospital information system.
2. System Realization and Test
1) Realization/testing environment
To construct the DMS proposed in this thesis, a server was installed between POCT equipment and a hospital data system, and a DMS server application, which was realized on the basis of the DMS framework design, was mounted on the server. Then, the overall system was constructed by connecting the client application to the DMS server through Ethernet. In this study, the implementation of the system was carried out as follows. The implementation of all the system was based on C# language, and .Net Framework 2.5 under Visual Studio 2005 development environment tools was used. The MS SQL Express database was used as the database of the DMS server. The operating system of the DMS client application was Microsoft Windows XP Professional Edition Service Pack 3, and the operating system of DMS Server Application was Microsoft Windows Server 2003 Enterprise Edition Service Pack 2.
The DMS server, client and hospital information system were connected to the same Ethernet environment, and three pieces of equipment were connected to the Ethernet environment with wire or wireless.
2) Tests
(1) Connection persistence and reliability verification test
The purpose of these tests was to confirm if the DMS could carry out the role as a bridge enabling the results generated by the equipment to be delivered quickly and accurately. To achieve this, the efficiency was verified by using two test factors in these tests.
The first factor was the average transmission time for results. This was used to calculate the gap between the time for result generation by the equipment and the time when the relevant results are received at the DMS, so that the efficiency of connection persistence may be verified in terms of the average numerical value.
The second factor was the result reception rate. This percentage value was calculated from the proportion of the number of results generated by the equipment and the number of results received by the DMS. This factor was used to verify the connection reliability. The characteristic of mobile equipment was reflected by applying a blocking event three times a day as a main variable.
During the 2-week test period, a piece of sample was measured a result was generated every 10 minutes from 18:00 PM to 24:00 PM, and the result was transmitted to the DMS and a comparison system immediately after the result was generated. However, the equipment network was blocked once every two hours, and it was reconnected to the equipment 5 seconds later. Also, the equipment was disconnected from each system when the next result was being measured, was connected manually to make it communicate.
(2) Verification test for data integrity and interoperability
The purpose of this test was to comprehensively integrate the data in different types of protocols from various types of equipment, so that the efficiency of data integrity may be confirmed. This test is designed to determine whether it is possible to deliver orders and transmit or receive data by delivering integrated data after it is transformed into the type of message used in a hospital information system. This test was also used to verify of the utility of the system by confirming if the system can be integrated efficiently as a single system when other equipment is added.
3. System Evaluation
1) Efficiency evaluation regarding connection persistence and reliability
This test evaluated efficiency in terms of connection persistence and reliability by comparing the transmission time and data collection rate results between the existing system and the DMS.
Firstly, the efficiency verification regarding the connection persistence may be confirmed through average result transmission time. The graph in Figure 4 shows the result transmission time per result generation time. The red dots represent the result transmission time received by the proposed DMS. Usually, the following results were received within 60 seconds after the system was disconnected. On the contrary, when results were collected in the other system, it was confirmed that it usually took more than 600 seconds despite the connection by hand.
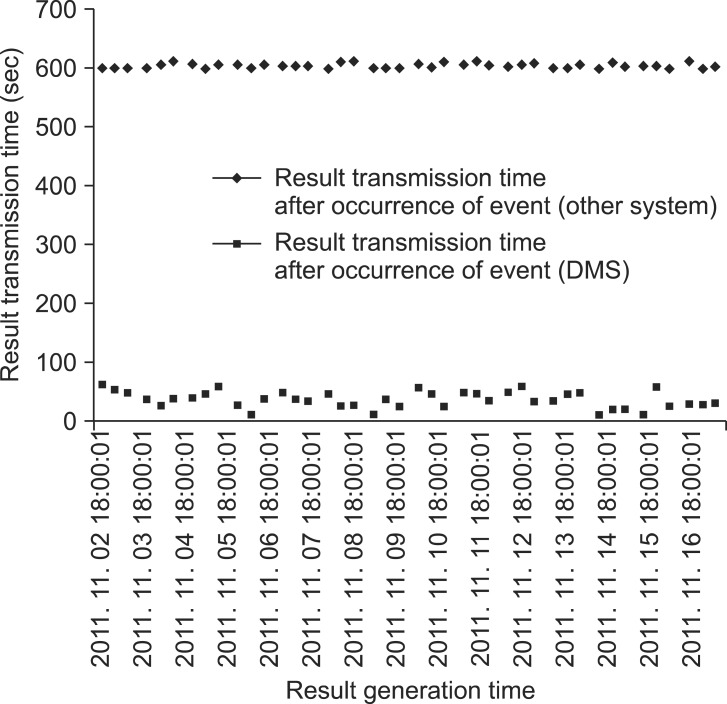
The graph of results transfer time immediately after event (disconnect). DMS: data management system.
Then, the data collection rate was confirmed by verifying efficiency in terms of connection reliability. In the test, the reception rate and average result transmission time of the DMS and the other system were analyzed and compared; we confirmed that the reception rate of the DMS was higher than the other system by 30%. Also, it is expected that the DMS will provide higher efficiency in an actual hospital environment because the results of DMS were obtained right after the network was blocked, but the results from the other system were obtained by securing the connection by hand.
2) Efficiency evaluation for data integrity and interoperability
This test was carried out to verify efficiency in terms of data integrity. In this test, the major evaluation standard was to confirm if it was possible to integrate various types of equipment in a single system and if it was possible to carry out efficient integration of additional equipment. The results confirmed that various types of equipment could be integrated into a single system. In particular, it was found out that the relevant equipment could be integrated by applying simple rules to the added equipment after the system was constructed.
In this way, the possibility to integrate multiple types of equipment into a single system, or integrate additional equipment in an easy way has many merits. Especially when introducing POCT equipment to a hospital and making effort to obtain interoperability with the existing system, it is possible to achieve greater time efficiency. It is also expected that the complexity of system will be reduced.
The next is a test was carried out to verify of interoperability. In this test, the major evaluation standard was to confirm if the integrated data can be delivered after transformation into an HL7 message used in the hospital information system. After the data was generated by each piece of equipment, it was transformed into a standardized type of message, such as LIS2-A2 and HL7.
In particular, it was confirmed that the data generated by a blood analysis device, AVL 9130, could be generated in a standardized type of message according to the rule-based mapping technique, though the data was in a message type that did not follow the standards. Also, it was found that data generated in this way could be transferred to the hospital information system application, or the data could be confirmed through the DMS client application. Such integration, the generation of standardized message, and transfer functions play an important role in which the DMS connecting the POCT equipment and hospital information system ensures interoperability between the two nodes.
3) Comparative evaluation between DMS and other systems
It was thought that proving the efficiency of the proposed system through the comparative analysis of a single system could be affected by a subjective point of view. Therefore, objectivity in evaluating the efficiency of the proposed DMS in terms of connectivity, integration, and interoperability was ensured by comparative test with multiple systems. Table 1 shows the list of systems used in the comparative tests together with the test results.

Comparison with other systems
We found that the company manufacturing the POCT equipment provides the following system additionally. However, connectivity, integration, and interoperability were not yet sufficient in integrating mobile equipment like POCT. This was proved through a comparative analysis with our system. And as for the order generation function, which is an important function used for integration of POCT equipment, we found out that most systems depend on manual generation or do not have such functions. However, it was confirmed that our system addressed problems related to loss of results and omission of insurance claims, which may happen in actual hospitals, by providing the automatic order generation function. Finally, it was possible to objectively assess the efficiency of the DMS proposed in this thesis through such comparative tests.
IV. Discussion
To raise the quality of patient service, hospitals are currently introducing POCT equipment. However, the operation of POCT equipment is carried out on condition that the equipment maintains interoperability with the existing hospital information system. In this study, the problems related to introduction of POCT equipment into an existing hospital information system were divided into three categories, namely, connectivity, integration, and interoperability. To address these problems, we designed and realized a DMS that can ensure the sharing of information between POCT equipment and an existing hospital information system. Comparative test results showed that the result of our system could go beyond each evaluation standard, and the system showed much higher efficiency in comparison with other systems. Thus, it is expected that implementation of the proposed DMS will ensure the advantages of POCT equipment will gain a foothold on which hospitals may provide better medical services and improve the quality of patient services.
In this study, the clinical equipments in a hospital was used, and the research scope was limited to TCP/IP service through wire/wireless LAN in terms of the connection of physical interface. Recently, many-sided changes have occurred in medical services due to the fast growth of the u-Health care industry.
Therefore, the equipment offering physical and logical interface are provided. Consequently, the problems related to connection and integration have be put at the top of agenda that shall be dealt with in the medical industry. In the future, we are going to carry out a study to improve the interoperability of equipment used in u-Health care services based on the DMS designed in this thesis.
Acknowledgments
We are grateful for the support of relevant authorities as this study has been carried out on the basis of the support of the Advanced Technology Center.
Notes
No potential conflict of interest relevant to this study was reported.