I. Introduction
Increased interest in disease prevention and health promotion is one of the significant changes in relation to healthcare consumption. The leading cause of death has been shifted from infectious diseases to chronic diseases in Korea due to lifestyle changes, an enhanced level of medical care, greater accessibility of medical services, and other factors [1]. Thus, treatment-oriented healthcare has shifted toward disease prevention and health promotion.
In recent years, regular health screening has become popular as the number of health promotion centers has increased. Health promotion has been defined by the World Health Organization's 2005 Bangkok Charter for Health Promotion in a Globalized World as "the process of enabling people to increase control over their health and its determinants, and thereby improve their health" [2]. The number of health promotion centers has been increased to promote healthcare from the aspect of preventive medicine domestically. These services are being provided by health checkups or promotion centers as conventional medical services are diversified [3]. The managerial performance of such services preserves losses which are generated from other hospital departments, and it plays a crucial role in overall hospital management [4]. For these reasons, many medical institutions have set up physical examination and health promotion centers to provide health screening service.
As of April 2012, eight hundred and forty-three health promotion centers operated nationwide [5]. Due to intensifying cut-throat competition among health promotion centers, providing diversified customer-tailored services has been highlighted by analyzing customer's needs for hospitals to hold a dominant position. Escalating competition among health promotion centers changed the trend of patients visiting hospital voluntarily.
Competition among businesses is intensifying as customers' demands have diversified. Hence, many businesses are pushing to build effective relationships with customers by meeting their needs. Likewise, finance, service, distribution, communication, and other various industries are making every effort to strengthen customer relationships by introducing customer relationship management (CRM) systems.
The CRM system is a marketing technique that focuses on securing and appealing to loyal customers by providing differentiated service through customer categorization to underscore the importance of customers in the management field [6]. The application of CRM systems is acknowledged to be beneficial in finding new customers, enhancing customer value, maintaining customers, and attracting customers with high-return [7,8]. Reichheld and Sasser [9] suggested that the net income of service businesses would be increased from 25% up to 85% if the attrition rate of clients could be decreased by at least 5%.
The CRM system has been used as a way to maximize customer satisfaction by identifying customer needs and providing qualitative healthcare services based on patient preferences [6]. A favorable relationship between healthcare providers and patients not only improves customer satisfaction but also enables effective communication between them. Moreover, it will help improve the quality of health overall, and assist in the effective management of chronic diseases [10,11]. The CRM system also could create higher profits for hospitals. For these reasons, many healthcare providers have predominantly built CRM systems in health promotion centers. Although the importance of marketing and customer management has been underlined in health promotion centers, few studies have been conducted on the current domestic state of CRM system utilization and its accomplishment.
Therefore, we attempted to establish an information system success model for CRM systems to find the crucial factors of CRM systems in health promotion centers. This study would provide both performance indicators and success factors of CRM systems in relation to actual users of such systems in health promotion centers.
1. Theoretical Background
Although assessing the performance of information systems is difficult due to their diverse characteristics, it is a crucial part of the process in the information resource management of organizations. Major studies on the performance of information system are summarized as follows. DeLone and McLean [12] proposed a model assessing the effect of information systems in six sectors including system quality, information quality, use of system, user satisfaction, individual impact, and organizational impact.
Although DeLone and McLean received extensive support in the performance assessment of information systems and enormously influenced later studies [12], their study introduced many controversial issues at the same time. DeLone and McLean [13] proposed the modified information system success model, which adds the service quality area.
In 1995, Pitt et al. [14] proposed a revised model which adds the service quality of the SERVQUAL model to the information system success model of DeLone and McLean [13]. They proved that the SERVQUAL model used in marketing is applied in assessing the service quality of information system through an empirical study on information system service quality.
Seddon [15] pointed out the limitations in assessing information system performance inclined to technical areas and enforced user characteristics, such as the participation and spontaneity of users. Moreover, he emphasized that perceived usefulness is more desirable in assessment rather than usage when the use of information is not spontaneous.
After conducting a study on 181 subjects in financial businesses and 267 information system service users in 1997, Myers et al. [16] concluded that system quality, information quality, and service quality influence user satisfaction. Moreover, they emphasized that performance needs to be assessed from various aspects, and the effect of each perforamance factor should be verified by distingusihing individual performance, group performance, and organizational performance as dependent variables.
Meanwhile, Yusof [17] attempted to extend the existing in formation system assessment model to the medical field. The study introduced a new evaluation framework; human, organization, and technology-fit (HOT-fit). Although Yusof's HOT-fit framework was proposed to be applied to the fundus imaging system used in primary medical care facilities of the National Health Service in the UK, no further related studies have been made [17].
II. Methods
2. Research Methods
Although the study searched publically released statistics on health promotion centers for the selection of subject institutions, no related data were found. Consequently, the 40 health promotion centers were selected from nationwide tertiary hospitals designated by the Ministry of Health and Welfare from 2012 to 2014. We requested permission to carry out a survey at the selected health promotion centers of the selected hospitals by informing the directors of each hospital of the purpose of the study. However, only 13 of these health promotion centers were included where they answered that the CRM system had been introduced. Therefore, questionnaires were distributed to the CRM system users working in these 13 health promotion centers, and 245 questionnaires were withdrawn (collection rate, 86.27%). We used 243 collected questionnaires for the analysis, excluding two copies with insincere answers. All responses were measured using a 5-point Likert scale.
The PASW Statistics ver. 18.0 (SPSS Inc., Chicago, IL, USA) and AMOS ver. 18.0 statistical packages (SPSS Inc.) were used for the data analysis. The data analysis comprised two phases. In the first phase, the demographic characteristics of subjects were identified using the PASW Statistics ver. 18.0, and then factor analysis and reliability analysis were performed on survey items of independent variables. In the second phase, path analysis was carried out to identify the goodness-of-fit and path coefficient of correlation analysis and the study model using the AMOS ver. 18.0.
3. Research Hypotheses
1) System characteristics
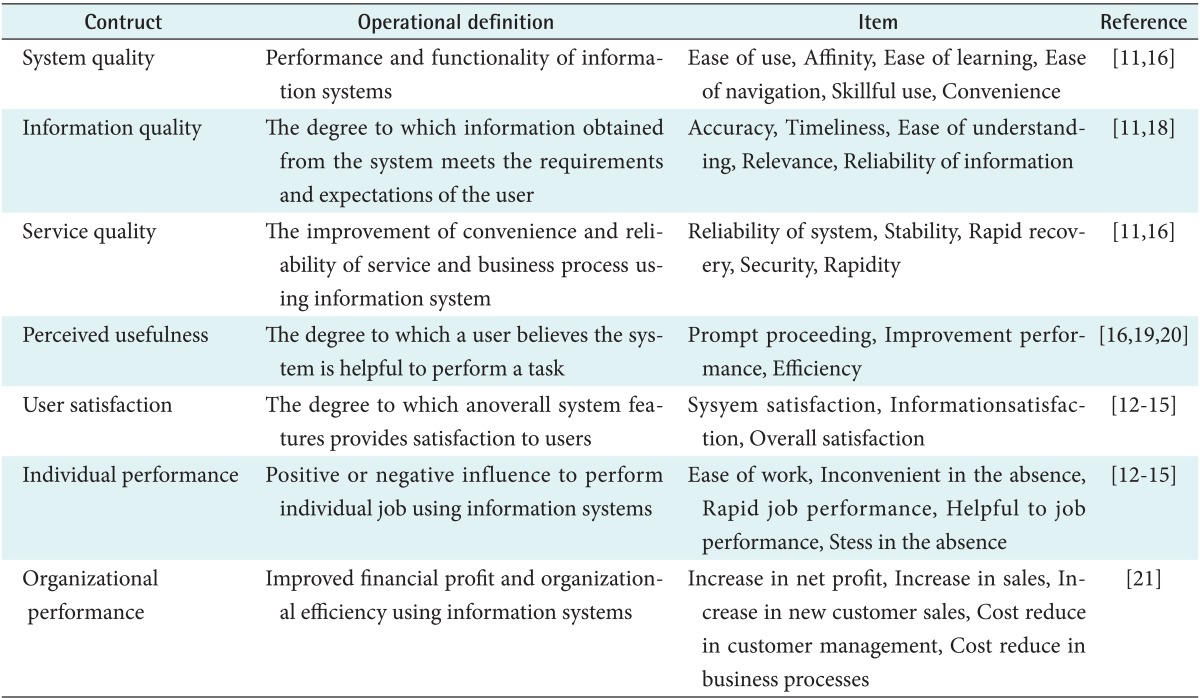
System characteristics include the technical factors of information systems. In this study, the system characteristics included system quality, information quality [12], and service quality [13,14].
The system characteristics of information systems have a positive impact on the effectiveness of the user. System characteristics, which include system quality, information quality, and service quality, affect the behavioural intention to use the system and user satisfaction. The system characteristics also affect both individuals and organizations. Finally, the system characteristics affect net benefits [13]. In addition, system characteristics affect the usage of and user satisfaction with information systems [22,23]. Kim et al. [24] suggested that information quality has a relationship with user satisfaction.
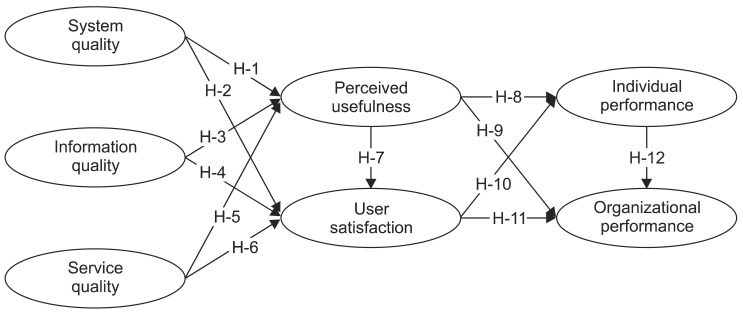
Based on previous studies, we predicted that CRM system characteristics have a relationship with utility characteristics, which include perceived usefulness and user satisfaction. Accordingly, we propose the following six hypotheses.
H1: System quality will have a positive impact on perceived usefulness.
H2: System quality will have a positive impact on user satisfaction.
H3: Information quality will have a positive impact on perceived usefulness.
H4: Information quality will have a positive impact on user satisfaction.
H5: Service quality will have a positive impact on perceived usefulness.
H6: Service quality will have a positive impact on user satisfaction.
2) Utility characteristics
User satisfaction is a useful measure by which to assess the effectiveness of information system users [25]. Some previous studies have proposed that utility characteristics should include usage and user satisfaction. However, other studies have emphasized that the performance of an information system should be evaluated in terms of its perceived usefulness rather than actual usage in cases in which system acceptance is involuntary [14,16]. User utility characteristics also include perceived usefulness and user satisfaction [15,18]. System acceptance of CRM systems in health promotion centers is involuntary; therefore, based on previous studies, we define user utility characteristics to include the perceived usefulness of a system and user satisfaction.
3) System performance
Information systems include a variety factors in organization. The performance of information systems cannot evaluate separately. In this study, the considered performance factors included individual performance factors and organizational factors, based on previous studies [12,13,15,18]. We established four hypotheses related to the relationship between users utility, which included perceived usefulness and user satisfaction, and performance factors. Organizational performance was measured in terms of financial performance because it is difficult to measure performance created by information systems.
H8: Perceived usefulness will have a positive impact on individual performance
H9: Perceived usefulness will have a positive impact on organizational performance
H10: User satisfaction will have a positive impact on individual performance
H11: User satisfaction will have a positive impact on organizational performance
Information performance was measured in terms of individual performance and organizational performance, according to many studies [12,14]. In this study, we posited a hypothesis about the relationship between individual performance factors and organizational performance factors to examine the relationship between performance factors.
III. Results
1. General Characteristics of Health Promotion Centers and Respondents
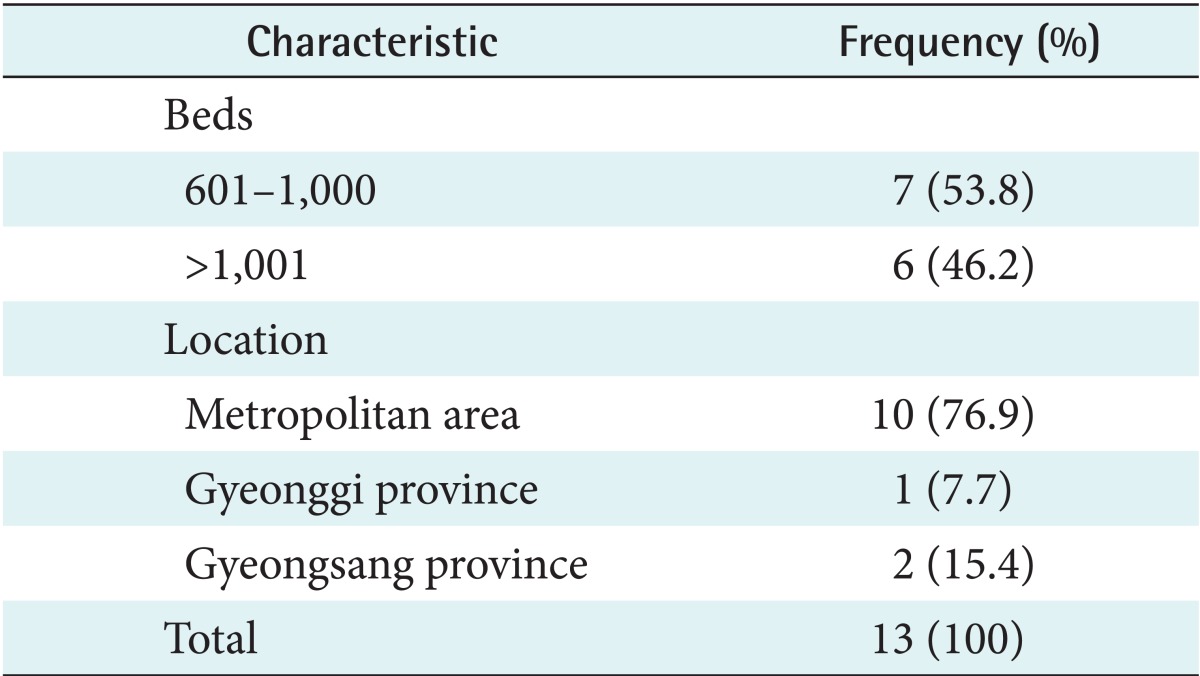
The characteristics of the health promotion centers considered in this study are shown Table 2. There were 7 centers (53.8%) with 601-1,000 beds and 6 centers (46.2%) with more than 1,001 beds. Moreover, 10 hospitals (76.0%) were located in metropolitan areas, and three hospitals were located in non-metropolitan areas, that is, the South Gyeonggi (7.7%) and Gyeongsang Provinces (15.4%), respectively.
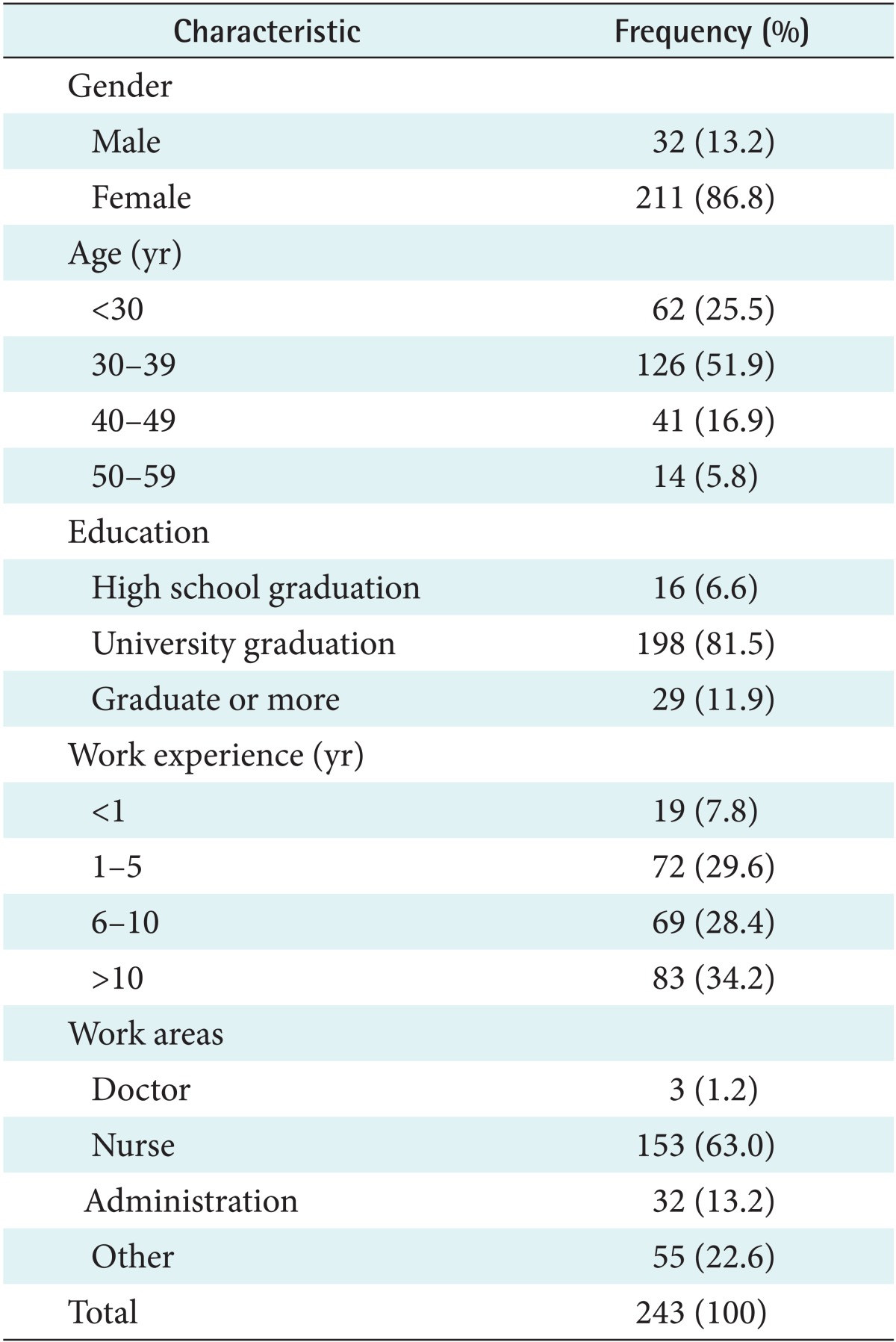
The demographic characteristics of respondents are summarized in Table 3. The 13.2% of the respondents were men and 86.6% were women. By age, 62 respondents (25.5%) were below 30 years of age, 126 respondents (51.9%) were between 30-39 years of age, 41 respondents (16.9%) were between 40-49 years of age, and 14 respondents (5.8%) were between 50-59 years of age. By educational background, high school graduates were 16 (6.6%), college graduates were 198 (81.5%), and respondents above a post-graduate degree were 29 (11.9%). By work experience, 19 respondents (7.8%) had less than a year of work experience, 72 (29.6%) had two to five years of work experience, and 83 (34.2%) had six to ten years of work experience. By work field, three respondents were doctors, 153 respondents were nurses, 32 respondents were administrative staff members, and 55 respondents were other workers.
2. Reliability and Validity
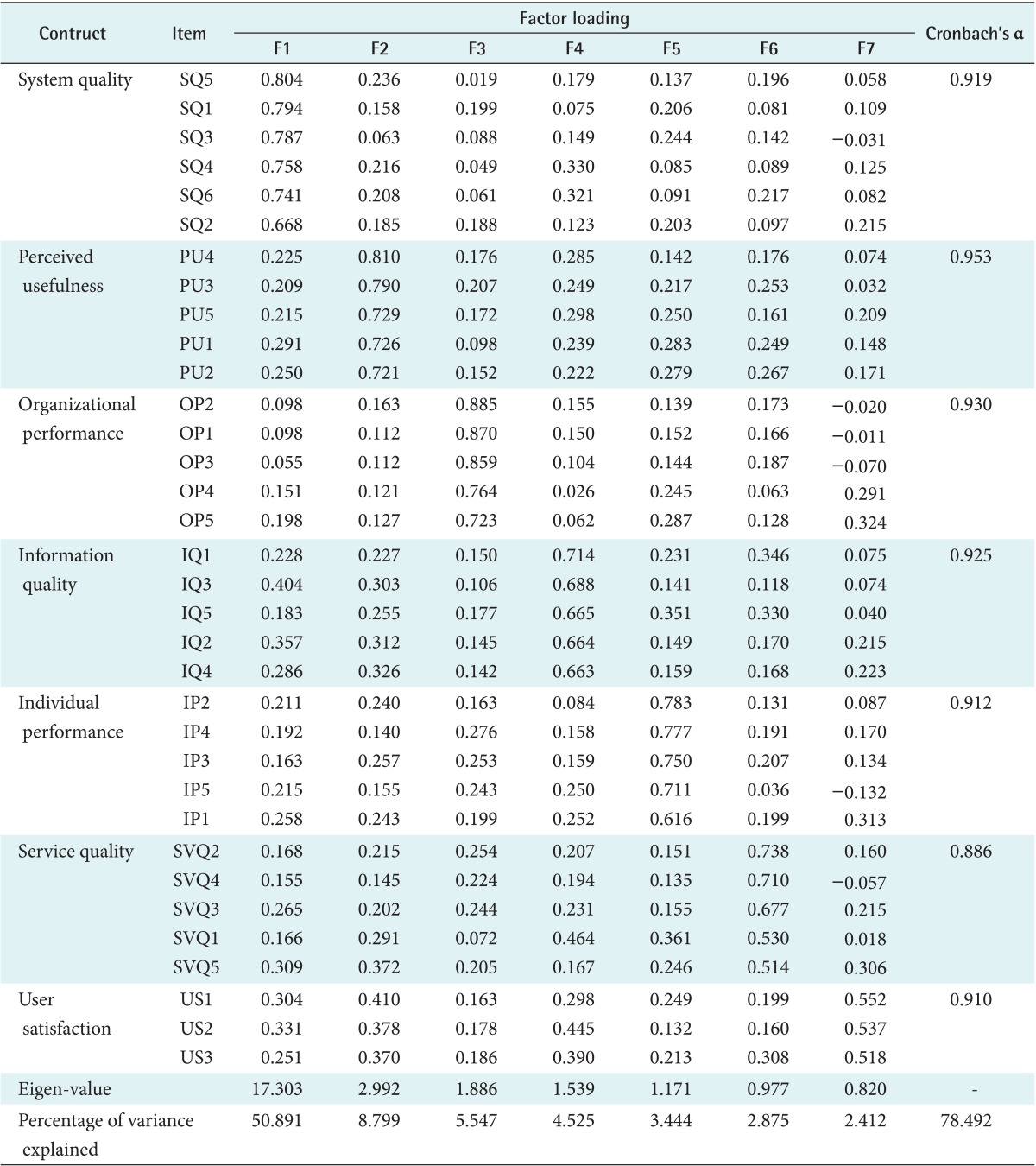
First, the validity of the evaluating factors was tested through exploratory factor analysis. The study used the varimax, the most commonly used orthogonal factor rotation. Cronbach's α value, representing the average value of repeatedly measured data, was calculated to assess the reliability. Each survey item was considered to exhibit internal consistency if it expressed reliability of 0.886 or above. Thus, the factors comprising this study model are thought to have high reliability and internal consistency [27]. The results of the exploratory factor and reliability analyses are shown in Table 4.
Second, we tested for reliability and validity using confirmatory factor analysis (CFA).
For the measurement model, CFA revealed a good model fit, chi-square/degree of freedom (χ2/df, 2.66), goodness-of-fit index (GFI, 0.777), adjusted GFI (AGFI, 0.830), normalized fit index (NFI, 0.865), comparative fit index (CFI, 0.919), and root mean square residual (RMR, 0.04) [23]. In this study, these were within acceptable levels.
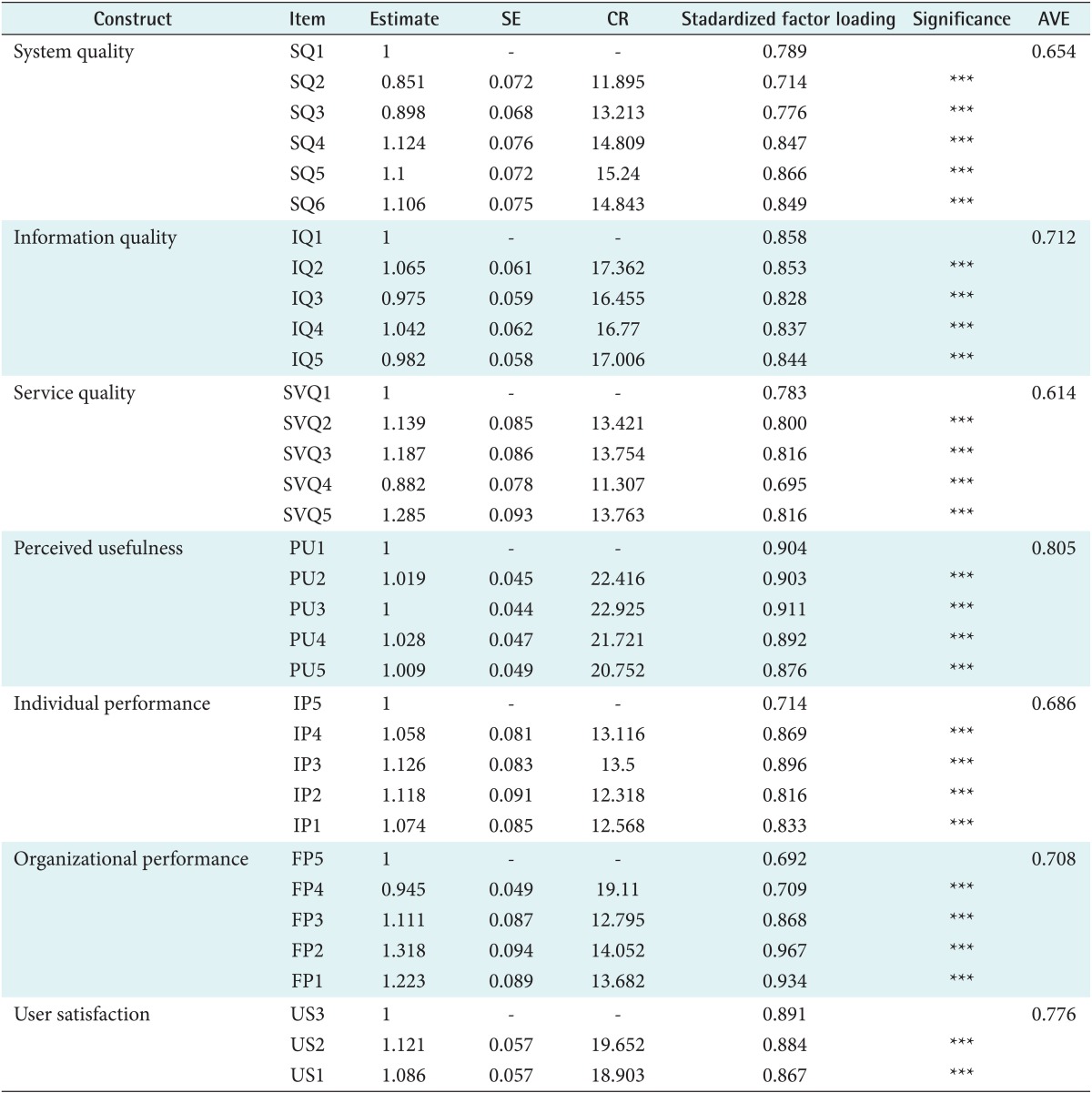
The convergent validity of each construct was evaluated (Table 5). The criterion for assessing adequate convergent validity was the average variance extracted (AVE), which is the average variance that is shared between a construct and its measures. Convergent validity is adequate when constructs have an AVE loading greater than 0.5, which means at least 50% of the measurement variance was captured by the construct. All constructs demonstrated AVE scores greater than 0.5, which is the minimum recommended score.
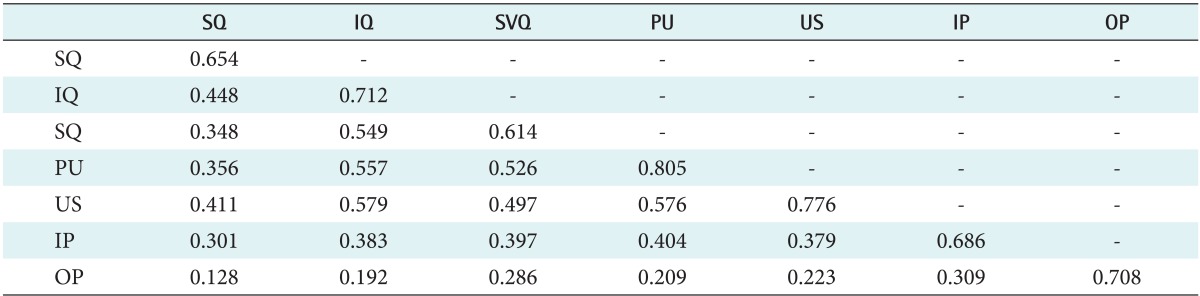
Following the convergent validity assessment of the measurement model, the discriminant validity of each construct was evaluated. Table 6 presents the AVE for each construct and the square of the correlations, between each construct and the others. The results support the discriminant validity of each of the constructs, as the AVE of each was greater than that of the corresponding inter-construct squared correlation (Table 6).
3. Suitability of Research Model
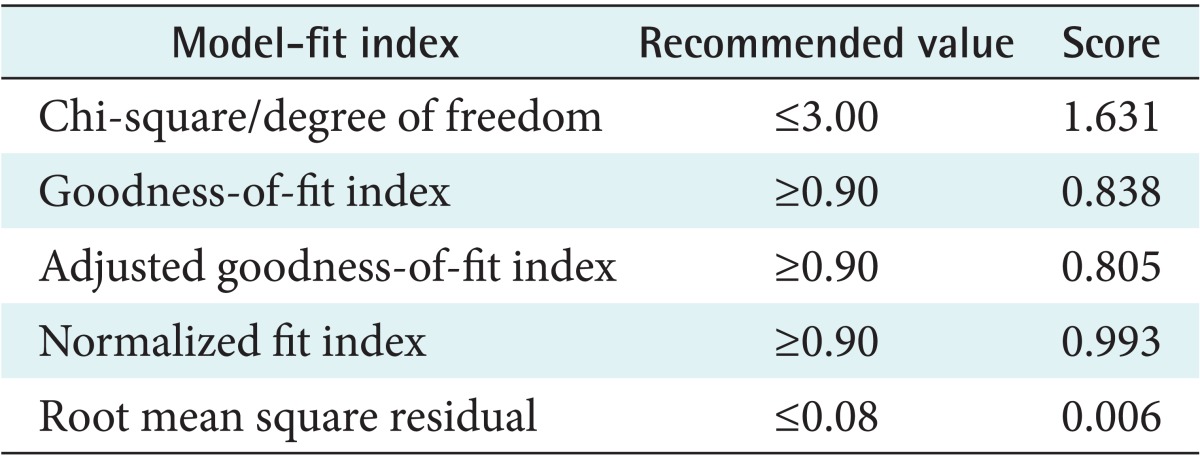
The goodness-of-fit of the proposed model was assessed using the GFI, AGFI, NFI, RMR, and CFI [23]. The goodness-of-fit of social science was determined based on GFI (≥0.9), AGFI (≥0.9), RMR (≤0.08), and NFI (≥0.9). The GFI and AGFI values of about 0.80 and 0.89, respectively, generally indicate acceptable model fit. The GFI and AGFI values in this study exceeded 0.90, which suggests a relatively good overall fit for the model.
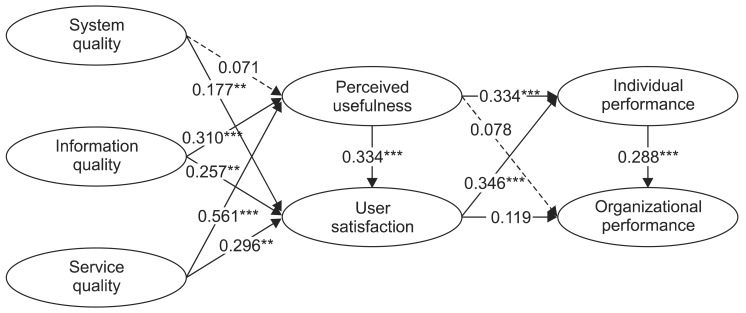
Figure 2 shows the causal relationship among factors determined by conducting the path analysis of each factor. According to the test results of the structural model, the goodness-of-fit statistics and coefficients were χ2/df, 1.631, GFI, 0.838; AGFI, 0.805; RMR, 0.006; and NFI, 0.993; which are quite close to the recommended standard of goodness-of-fit (Table 7). In this study, neither the GFI nor the AGFI values satisfied the recommended threshold of 0.9 or greater. However, the GFI and AGFI values may be overly influenced by the size of sample [28]. For this reason, some studies have recommended the use of less sensitive fit indices, such as GFI, AGFI [29]. Therefore, the GFI and AGFI values were below 0.9, but these values may be acceptable. The overall goodness-of-fit levels in the study are thought to be acceptable in anticipating the relationships among variables in hypothesis testing.
4. Hypothesis Testing
This study tested hypotheses presenting the relationships among system characteristics, user, and performance of a CRM system evaluating areas in health promotion centers. Among 12 hypotheses, 9 hypotheses were chosen excluding three hypotheses at a significance level of 0.05. The results are shown in Table 8. Information quality (path coefficient, 0.310) and service quality were found to have a positive influence on perceived usefulness. User satisfaction was shown to be affected by system quality (path coefficient, 0.177), information quality (path coefficient, 0.257), and service quality (path coefficient, 0.296). Perceived usefulness (path coefficient, 0.334) showed a positive effect on user satisfaction. Perceived usefulness (path coefficient, 0.334) and user satisfaction (path coefficient, 0.346) had a positive influence on individual performance. On the other hand, both perceived usefulness (path coefficient, 0.078) and user satisfaction (path coefficient, 0.119) had no influence on organizational performance. Finally, individual performance (path coefficient, 0.288) exhibited a positive effect on organizational performance.
IV. Discussion
The CRM system in health promotion center has been known as a significant system affecting the competitiveness of healthcare providers. We examined the performance of the CRM system and the effect of system characteristic factors on individual and organizational performance. The study has reached the following conclusions based on the research results.
First, information quality and service quality were found to have an influence on perceived usefulness among the factors in the system characteristic area. Moreover, system quality, information quality, and service quality all had effect on user satisfaction. The outcomes show good agreement with the results of previous studies that have underscored service quality in the performance of other information systems, including DeLone and McLean [13], Pitt et al. [14], and Seddon [15]. Information quality and service quality, in particular, influenced both perceived usefulness and user satisfaction unlike system quality in this study. The results imply that service quality providing qualitative information rather than the system itself positively influences user satisfaction and perceived usefulness. Therefore, enhancing user services and providing constant high-quality content are crucial to raise the performance of the system.
Second, although the relationship between the system and organizational performance has been a critical issue in evaluating the performance of information systems, performance evaluation had not been attempted due to complexity. When the study assessed the performance of CRM system in hospitals, perceived usefulness and user satisfaction were found to directly influence individual performance in terms of work efficiency and task performance availability; thus, these factors were found to indirectly affect organizational performance ultimately. These results confirm that the CRM system plays a significant role in the competitiveness of health promotion centers.
The implications of this study are summarized as follows.
First, the study broadened the scope of research by applying the hospital information-centered information system performance model as the CRM system evaluation model by highlighting the need to assess the CRM system and practically analyzing evaluating indicators. Although the CRM system was operated separately from ordinary hospital information systems, our results show that the same evaluation standards can be applied in the performance assessment. Second, the study scientifically laid the foundation for evaluating the CRM system in health promotion centers and practically provided useful guidelines for CRM system operation by obtaining and evaluating data from actual CRM system users and determining the factors affecting the system performance. Third, the study confirmed the validity of the study model by empirically testing the introduced model and hypotheses through statistical methods. Fourth, the performance of the CRM system needs to be eventually affiliated with organizational performance, implying that the proposed factors need to be taken into consideration in the introduction and expansion phases of the CRM system in every evaluation area.
The study results indicate that achieving competitiveness is crucial from the design phase of the CRM system to the system characteristic area. Since perceived usefulness and user satisfaction influence individual performance as well as organizational performance, sustainable management is essential to increase usefulness and user satisfaction. Moreover, all of the system characteristic areas affected user satisfaction and user satisfaction affected individual performance. Hence, the quality of information systems needs to be maximized to improve user satisfaction. Since organizational performance was evaluated in terms of financial performance as perceived by employees, strengthening individual performance ultimately leads to enhanced financial performance of organizations.
Despite such important contributions of this study, it has the following limitations.
First, supplementary studies are essential in the future since individual characteristics of users were not taken into account. When different characteristics and factors affecting the usefulness and performance of the CRM individual users are further examined, a broader CRM system will be able to introduce success factors. Second, extended studies should be performed that would include more hospitals as subjects and would reflect the size or characteristics of hospitals. Third, collecting data on the characteristics of hospitals was restricted due to the confidentiality of information. No hospital disclosed the number of monthly examinees in their healthcare centers or the operational method of their information systems. An extended study would be able to identify the relationship between the size and characteristics of hospital when more data is available, since hospital size is distinguishable by the number of examinees. Furthermore, when extended studies are performed reflecting the operational method of information system on factors affecting the performance, a broader CRM system will be able to introduce success factors.
A better and more appropriate CRM system will be established in the actual circumstances of health promotion centers when more studies are carried out that overcome the above limitations.