Challenges and Practical Approaches with Word Sense Disambiguation of Acronyms and Abbreviations in the Clinical Domain
Article information
Abstract
Objectives
Although acronyms and abbreviations in clinical text are used widely on a daily basis, relatively little research has focused upon word sense disambiguation (WSD) of acronyms and abbreviations in the healthcare domain. Since clinical notes have distinctive characteristics, it is unclear whether techniques effective for acronym and abbreviation WSD from biomedical literature are sufficient.
Methods
The authors discuss feature selection for automated techniques and challenges with WSD of acronyms and abbreviations in the clinical domain.
Results
There are significant challenges associated with the informal nature of clinical text, such as typographical errors and incomplete sentences; difficulty with insufficient clinical resources, such as clinical sense inventories; and obstacles with privacy and security for conducting research with clinical text. Although we anticipated that using sophisticated techniques, such as biomedical terminologies, semantic types, part-of-speech, and language modeling, would be needed for feature selection with automated machine learning approaches, we found instead that simple techniques, such as bag-of-words, were quite effective in many cases. Factors, such as majority sense prevalence and the degree of separateness between sense meanings, were also important considerations.
Conclusions
The first lesson is that a comprehensive understanding of the unique characteristics of clinical text is important for automatic acronym and abbreviation WSD. The second lesson learned is that investigators may find that using simple approaches is an effective starting point for these tasks. Finally, similar to other WSD tasks, an understanding of baseline majority sense rates and separateness between senses is important. Further studies and practical solutions are needed to better address these issues.
I. Introduction
The use of acronyms and abbreviations in both the biomedical and clinical domains is pervasive and increasing rapidly [1,2,3,4,5]. In clinical medicine, one of the main impetuses for this increasing use of acronyms and abbreviations is the fast-growing adoption of Electronic Health Record (EHR) systems resulting in the proliferation of electronic clinical documents. In addition to electronic clinical notes that are traditionally created by dictation and transcription, many clinical notes are now manually created within a time-constrained clinical work environment in which clinicians type or enter notes fully or use a semi-structured or templated document entry system. This often results in the use of shortened word forms that are frequently ambiguous and present a problem for subsequent information retrieval from EHR systems and potentially can lead to patient safety issues [6,7,8].
Development and improvement of automated techniques to resolve the sense of acronyms and abbreviations in clinical text is an important challenge for medical natural language processing (NLP), and it is considered an essential component for automated medical NLP systems [3]. Acronym and abbreviation sense resolution is considered a special case of word sense disambiguation (WSD) [9,10,11]. While interpreting the specific meaning of acronyms and abbreviations within a sentence is often easy for a human reader, this process is non-trivial for a machine [10,11]. In general English, studies have demonstrated that humans can properly resolve the meaning of most acronyms and abbreviations even if only given a very limited context of five words with the acronym or abbreviations in the central position [12,13]. Machine learning techniques have been used extensively to address the problem of automatic WSD in the biomedical and general English domains. Supervised methods have also been demonstrated in analogous studies to be potentially well suited for clinical acronym disambiguation [1,4,14,15].
Although acronym and abbreviation WSD has been studied extensively in relation to biomedical literature, relatively little research has been devoted to WSD of acronyms and abbreviations within clinical notes. In biomedical literature, typically the first instance of a short form for the acronym or abbreviation occurs with long form as a parenthetical expression or vice versa (e.g., mucosal ulcerative colitis) [11]. Because clinical notes are informal in nature, the association of the long form and short form in clinical text is rarely observed [5,15]. Moreover, the development of automated approaches for the disambiguation of acronyms and abbreviations in clinical text is complicated by legitimate issues of patient confidentiality and privacy which represent significant barriers for sharing clinical notes for research purposes [3,16].
Up to now, there has been limited utilization of clinical document characteristics and clinical knowledge resources for automated techniques addressing clinical acronym and abbreviation WSD. This article discusses issues encountered in acronym and abbreviation WSD using clinical notes from a tertiary healthcare institution. We then propose possible practical solutions to these problems based on our experiences to date.
II. Methods
Clinical documents from the University of Minnesota-affiliated Fairview Health Services, including the University of Minnesota Medical Center and three additional hospitals in the Minneapolis metropolitan area, from a 5-year period were used as our corpus for this study. This corpus was composed primarily of dictated clinical notes which were subsequently manually transcribed and stored in electronic format. These documents included admission history and physical examinations, consultations, and discharge summaries.
Acronyms and abbreviations were identified by using a set of heuristic rules with regular expressions and Perl scripts. An acronym or abbreviation for this study was defined as a token consisting of capital letters, numbers, and symbols (period, comma, colon, or semicolon). If this word token had more than 500 occurrences in the corpus, it was considered a potentially clinically significant acronym or abbreviation. After these acronyms and abbreviations were detected, 500 random occurrences were selected within the corpus, along with the surrounding previous 7 tokens and subsequent 7 tokens. These extracted instances were presented to two physicians who participated in this study to manually annotate for the senses of acronyms and abbreviations. The annotated sense of the acronym or abbreviation was then used as the reference standard.
Our goal was to obtain the optimal feature selection method for automated machine learning (ML) techniques to disambiguate clinical acronyms and abbreviations. To do this, we extracted a number of potentially predictive features by utilizing resources and techniques from a number of disciplines including biomedical NLP, computational linguistics, statistics and clinical practice. The feature types that were explored included 1) bag of words (BoW), which is defined as the set of surrounding non-normalized word tokens of the targeted acronym or abbreviation; 2) biomedical concepts via the Unified Medical Language System (UMLS) concept unique identifier (CUI); 3) biomedical semantic information (the UMLS semantic type of each concept); 4) linguistic information with parts of speech; 5) term frequency with other statistical information; as well as 6) heuristic clinical note structure and title/section information. We implemented the BoW approach using the set of surrounding 14 non-normalized word tokens and excluded English stop words that do not hold significant semantic information. We used a standard list of 57 English stop words [17]. MetaMap [18] was utilized to obtain both UMLS CUIs and UMLS semantic types for the targeted 14 surrounding words with the targeted acronym or abbreviation. MetaMap automatically processes the text and performs normalization and stemming as well. We also grouped semantic information using the previously described 15 semantic groupings of UMLS semantic types [19] as a set of features with UMLS semantic type information. Lastly, we extracted section names using a combination of heuristic rules with regular expressions and then ensured proper grouping of equivalent sections using manual classification by a physician. For the purposes of this pilot study, linguistic and statistical features were not included in the initial set of experiments.
Several supervised ML algorithms through the Weka data mining package [20] were used on each of the feature sets. We explored the application of naïve Bayes, support vector machines (SVM), and decision trees. In Weka, the specific algorithms are NaiveBayes, LibSVM, and J48, respectively. For our evaluation, we relied on the 10-fold cross-validation functionality implemented in Weka to assess performance for each abbreviation or acronym set of samples. Performance for each set of features and ML algorithm was measured in terms of precision, recall, and F-measure.
III. Results
As part of the 'lessons learned', we present the challenges faced to date, as well as practical learning from ongoing experiments in order to develop an effective medical NLP module for WSD of acronyms and abbreviations from clinical documents.
1. Practical Difficulties with Using Clinical Text
In the initial phases of our research, some of the key challenges that we encountered originated from several broad areas, including 1) variation in format, structure, and proper use of language in clinical texts including the common use of sentence fragments; 2) a shortage of resources, tools, and knowledge based on clinical notes; and 3) privacy issues regarding the use of protected health information.
1) Challenge 1: Language, structure, and formatting
Because the primary function of clinical notes is to record medical information conveyed between clinicians as a form of communication and documentation, these notes are not created with the intention of re-use or for the purpose of helping researchers perform automated tasks, such as WSD of abbreviations and acronyms. Therefore, one primary difficulty encountered in our work was the lack of formal structure in notes and format standardization of documents in EHR systems within the error-prone clinical environment. For example, there are portions of many clinical notes with extraneous text, which is not helpful for WSD research purposes. This includes formatting at the beginning and end of documents, extra white space, and the informal use of tables. Sometimes these are institution-specific formatting issues particular to the local EHR environment.
Outside of these formatting issues, we found significant variation within clinical documents even at the section level. For instance, within a subset of four or five document types within our corpus, over 25,000 lexically unique section headers were encountered (even after normalization for capitalization). Furthermore, there were additional errors owing to the lack of spell-checking [21] or language/grammar mistakes. Dictation from voice transcription may also result in mistakes because of a misinterpretation of word meanings/intentions between the clinician's intended meaning and the interpretation by the transcriptionist. Additionally, clinicians often used sentence fragments instead of fully structured sentences for efficient communication. This custom may hinder automatic WSD research because the extracted features miss valuable information.
2) Challenge 2: Shortage of resources
Another significant issue involved the currently limited resources and knowledge for WSD research in the clinical domain. For example, there are only a few available clinical acronym and abbreviation datasets (e.g., datasets by Xu et al. [15] or Mayo Clinic set [14]). Currently, there are no comprehensive clinical sense inventories for large numbers of acronyms available. Furthermore, it is well known there is a bottleneck problem in knowledge acquisition when collecting data or aggregating valuable information. In other words, the significant time, cost, and effort of experts are indispensable to obtain useful knowledge.
3) Challenge 3: Privacy issues
Finally, maintaining privacy and security while allowing greater access remains a significant challenge for researchers wishing to utilize clinical notes. Patient confidentiality policies with the Health Insurance Portability and Accountability Act (HIPAA) are strict. Large corpora of clinical text have not been traditionally easily available to NLP researchers. Rare exceptions include several notable efforts, including the i2b2 challenges [22] and the University of Pittsburgh Medical Center (UPMC) de-identified clinical notes repository [23]. Even the i2b2 and the UPMC datasets are not free of restrictions and necessary regulatory approvals. Furthermore, researchers with potential access to clinical documents containing protected health information at their own institutions encounter significant political and regulatory issues in gaining access to these documents or sharing these documents [3,16]. Consequently, relatively little research has been done on acronyms and abbreviations in clinical notes compared to biomedical literature documents. At our institution, we were able to obtain Institutional Review Board (IRB) approval for our research and to work directly with our clinical partners at the hospital to perform this research.
2. Starting from Simple Approaches
To overcome some of these difficulties, our approach has been to utilize the available resources, tools, and knowledge of other interdisciplinary fields. Overlapping concepts of the biomedical fields and domain-independent approaches to analyzing English language usage from the linguistic or statistical fields are methods that are reasonable to start with that might work directly or with some adaptation to the clinical domain. For feature selection, we expected that the utilization of advanced/elaborate tools, techniques, and knowledge especially from the biomedical fields would be beneficial for automatic WSD research in clinical documents.
These tools, however, have not been optimized for use within the clinical domain. For example, in contrast to biomedical literature discourse, as previously mentioned, clinical documents have short forms that are rarely associated with long forms. Moreover, biomedical tools utilize sense inventories primarily derived from biomedical literature, often ignoring or missing important clinical senses. Liu et al. [24] reported that UMLS covers only 66% of acronyms and abbreviations with less than 6 characters in the clinical domain. Many times, at least one of the senses encountered in our corpus was not contained within available references, such as the UMLS [4,5,16,24] or biomedical sense inventories, such as Adam [25]. Also, biomedical tools and typical linguistic tools (i.e., tokenizers or POS taggers) may fail with clinical text, where statements are often fragmented, sometimes without proper sentence boundaries.
The balance between utilizing existing tools, some of which have limited options for modification, versus development of customizable tools, remains difficult. We have attempted to use existing established tools where available, and retrain these tools where possible with clinical text. We are also trying to understand where these resources succeed and fail in order to optimize the previous work of others and reuse these resources. Moreover, we are focusing our efforts in areas where highly-specific tools for medical text are needed. In these attempts, it seems that clinically-oriented approaches would be helpful. Adopting clinical cognitive flows from medical specialties, position in discourse, and section information may be helpful.
Using simple features with simple ML algorithms can be a reasonable starting point. As a starting point, we chose to use the BoW approach to feature extraction coupled with the SVM algorithm. BoW was found to produce a simple but effective feature set. In our research, BoW often demonstrated competitive results over other isolated features or combinations of feature sets when various ML algorithms were used. Table 1 depicts the clinical sense distribution of seven abbreviations from our set. Table 2 shows the performance of different feature sets with naïve Bayes, SVMs, and decision tree algorithms for each of the seven abbreviations. Moreover, the combination of all possible feature sets (BoW, CUI, semantic type, and section) deteriorates the performance of ML because of duplicate and unnecessary data diluting critical information for ML algorithms in our experience (not pictured). As such, combining heterogeneous information with the prevention of overfitting is necessary.
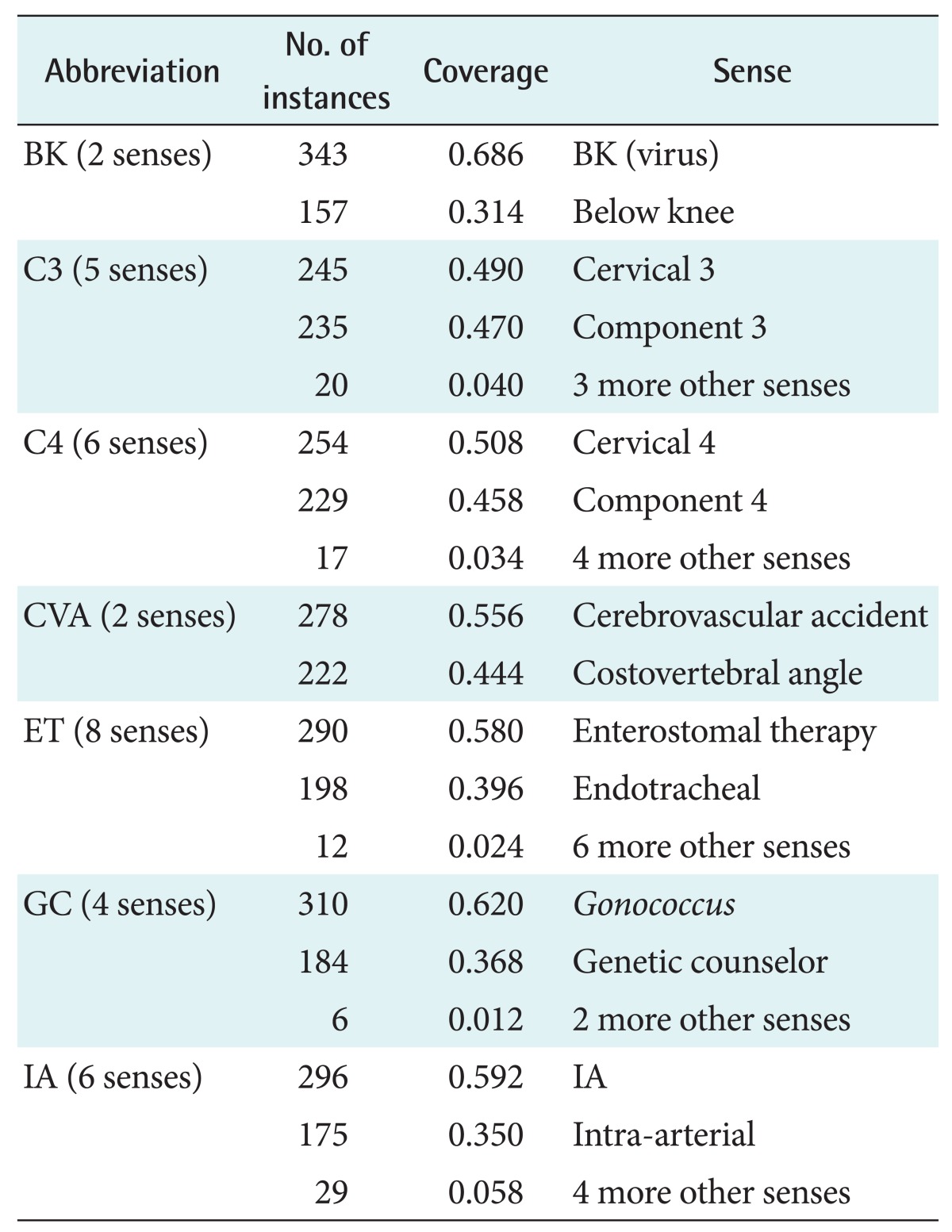
The sense distribution of abbreviations
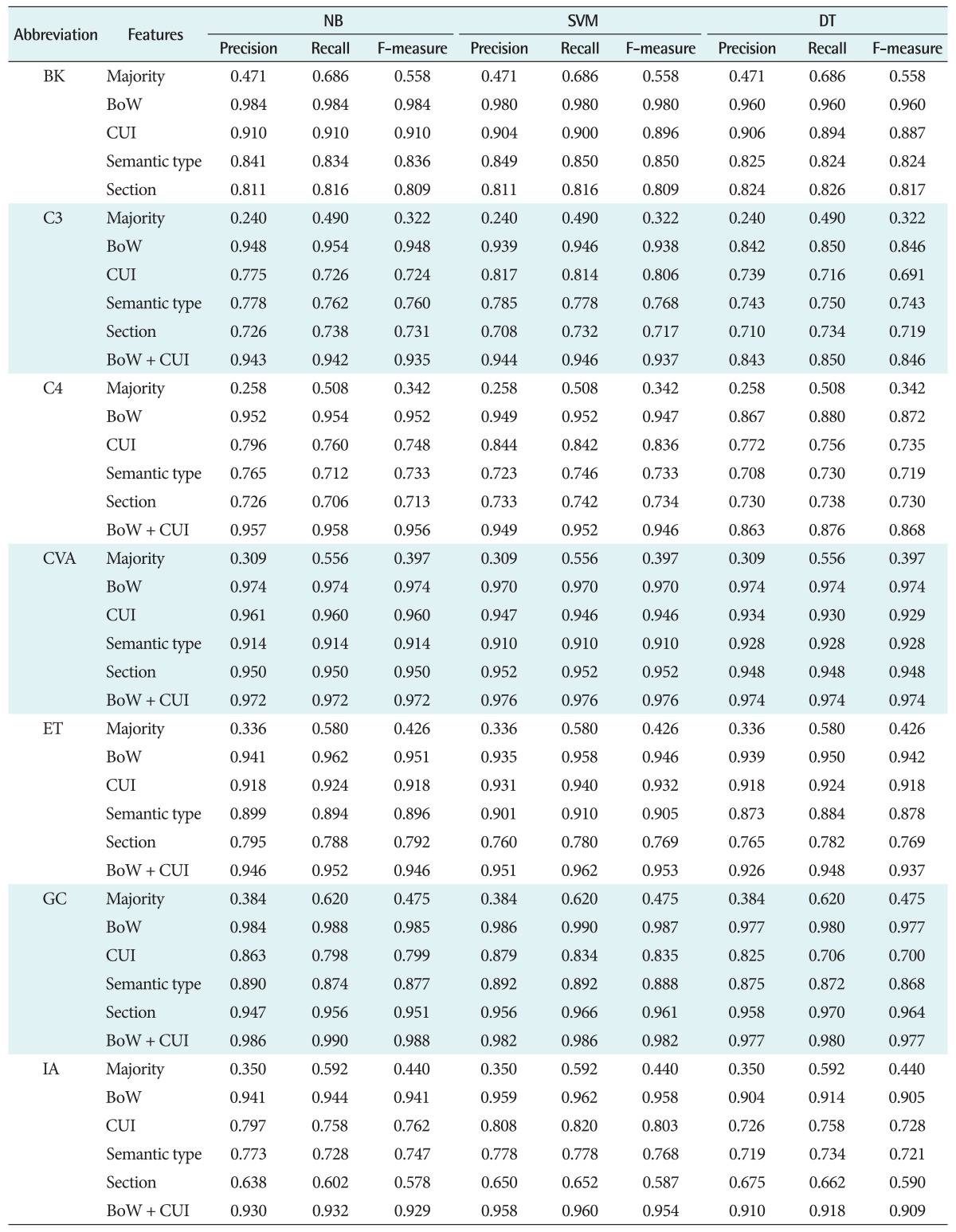
Precision, recall, and F-measure for abbreviations
3. Considerations in Assessing the Complexity of each Acronym and Abbreviation WSD Task
Even if we only use the simple BoW approach, it can be difficult to detect patterns when acronyms and abbreviations have different or skewed sense distributions. In our research to date looking at a large sample of acronyms and abbreviations within clinical documents, approximately half of these acronyms have only a single meaning (long form or sense) contained within a random moderate-sized sample of instances of each acronym in question (500 occurrences). After excluding acronyms with a single sense or a locally specific (specific to a particular institution) sense, we have found that biomedical sense inventories have a significant level of redundancy/synonymy between different long form expressions. This has required additional steps to reduce the redundancy of sense in sense inventories that needed to be taken prior to WSD [26].
After taking into account these factors, we observed performance patterns when grouping acronyms and abbreviations based on the majority sense rate. For instance, we found similar performance when the majority sense rate is relatively balanced because we are able to gather enough information about minority senses due to the availability of samples for each of the senses. On the other hand, gaining sufficient performance improvements can be difficult if distribution is skewed because the small number of samples for each of the minority samples may give insufficient information to help with proper disambiguation.
Another convenient consideration for researchers is an understanding of the relative degree of 'separateness' between senses. 'Well-separated' typically implies substantial semantic differentiation among senses [27]. However, 'well-separated' senses within a clinical text may also imply different uses within various sections of a single clinical note (e.g., different relative note location or different section). In principle, well-separated senses should then yield a higher accuracy for classification or clustering [4,28,29]. For instance, 'CVA' has two well-separated senses, 'cerebrovascular accident' and 'costovertebral angle'. In our experience, most of the feature sets for 'CVA' perform high accuracies, over 95%, when the SVM algorithm is used with only a few dozen samples during the training phases. Therefore, depending on the degree of separation, the necessary sample size for a training phase to achieve good performance might be estimated [4,30]. We have found to date a simple trend that acronyms or abbreviations having a single highly prevalent sense need more training samples than acronyms or abbreviations having evenly distributed senses to achieve significant performance improvements.
IV. Discussion
The proliferative use of acronyms and abbreviations in the clinical domain makes automatic sense disambiguation of acronyms and abbreviations for medical NLP systems an important ongoing challenge and area of research. For this pilot research, we studied WSD tasks for a few acronyms and abbreviations from clinical notes. From this, we have learned the following lessons: 1) practical difficulties with using clinical text that must be solved including language, structure and formatting issues, as well as lack of resources for clinical text and privacy issues; 2) starting from simple approaches, such as single features using well-known ML algorithms or using of well-separated senses is a sensible initial approach; and 3) to understand the performance of ML algorithms better, one should consider the distribution of senses of an acronym or abbreviation as well as the degree of separateness between senses and of usage between different long forms of an acronym. After these simple approaches, we need to customize tools and knowledge in order to harmonize clinical resources or to develop new tools from clinical fields.
According to several literature reviews examining biomedical and clinical documents, an optimal feature or set of features that will adequately address the disambiguation problem for biomedical or general English acronyms and abbreviation has not been found [9,16,30]. Due to these factors, accomplishing representative and optimal feature selection, a key step for classification or clustering, is an area of open research. Even if there are particular advantages and disadvantages of individual features within the clinical domain, there is no absolute superior feature identified for this task to date. Further study is needed with careful consideration of overfitting in clinical acronym and abbreviation WSD.
Acknowledgments
This work was supported by the American Surgical Association Foundation Fellowship, the University of Minnesota Institute for Health Informatics Seed Grant, and by the National Library of Medicine (#R01 LM009623-01). We would like to thank Fairview Health Services for support of this research. The authors also thank Serguei Pakhomov PhD for insightful comments.
Notes
No potential conflict of interest relevant to this article was reported.