I. Introduction
Over the past two decades, electronic health records have seen a major breakthrough in healthcare organizations, brought about by the rapid advancement of information and communication technology worldwide. Electronic dental records (EDRs), a subset of electronic health records, have been developed, implemented, and widely used among dental professionals in developed countries because of their proven usefulness and improvements in the quality of patient care [
1]. However, in developing countries, many challenges have been identified regarding the use of EDRs due to a number of barriers to their successful implementation in dental clinics [
23]. Implementation of EDR systems is challenging for dentists because most dental clinics are small; hence, they do not want to invest a lot of money in information technology [
4]. Moreover, they face further challenges such as ethical issues. For example, autonomy can be breached when data is shared or linked without the patients being informed, and trust can be lost when proper security measures are not applied [
5]. Most importantly, the doctor-patient relationship can be considerably impaired by the introduction of electronic health records in the dental office [
6]. Dentists who practice in Myanmar keep only basic patient records, which include limited information of patients’ health status, and patients are advised to bring their own records on subsequent visits. Only inpatient departments at two government hospitals keep full patient records. Dentists encounter a lot of problems related to paper-based dental records because patients often do not bring their paper-based records with them or lose them between visits, making it very difficult to obtain a reliable medical history for them. These problems could cause a serious weakening of the quality of patient care due to potential diagnosis or treatment errors [
7]. Therefore, most dentists in Myanmar wished to use EDRs to overcome these undesirable effects on patients. Nevertheless, implementation of a new electronic data-entry system in their dental clinics has been challenging for most dentists for a number of reasons, such as financial barriers, human resources barriers, knowledge barriers, and legal and regulatory barriers [
8]. In addition, even after the implementation of EDRs in dental clinics, paper-based patient records might still be superior to EDRs due to their simplicity of use and familiarity in most healthcare settings [
9]. Based on these points, it has been considered crucial to assess the benefits and drawbacks of paper-based dental records as well as barriers to, and perceptions around, the implementation of EDRs. There have been very few studies on the perception of EDR systems around the world [
10]. Furthermore, we did not find any work done in limited-resource settings, as in our study. We hypothesized that dental professionals in Myanmar were satisfied with currently using paper-based dental records, and this might influence their perceptions and intention to use the electronic dental record system. Therefore, this study aimed to measure user satisfaction regarding various aspects of paper-based dental records, views on EDRs, and perceived barriers to the implementation of EDRs among dental professionals practicing in the Yangon and Mandalay divisions in Myanmar.
II. Methods
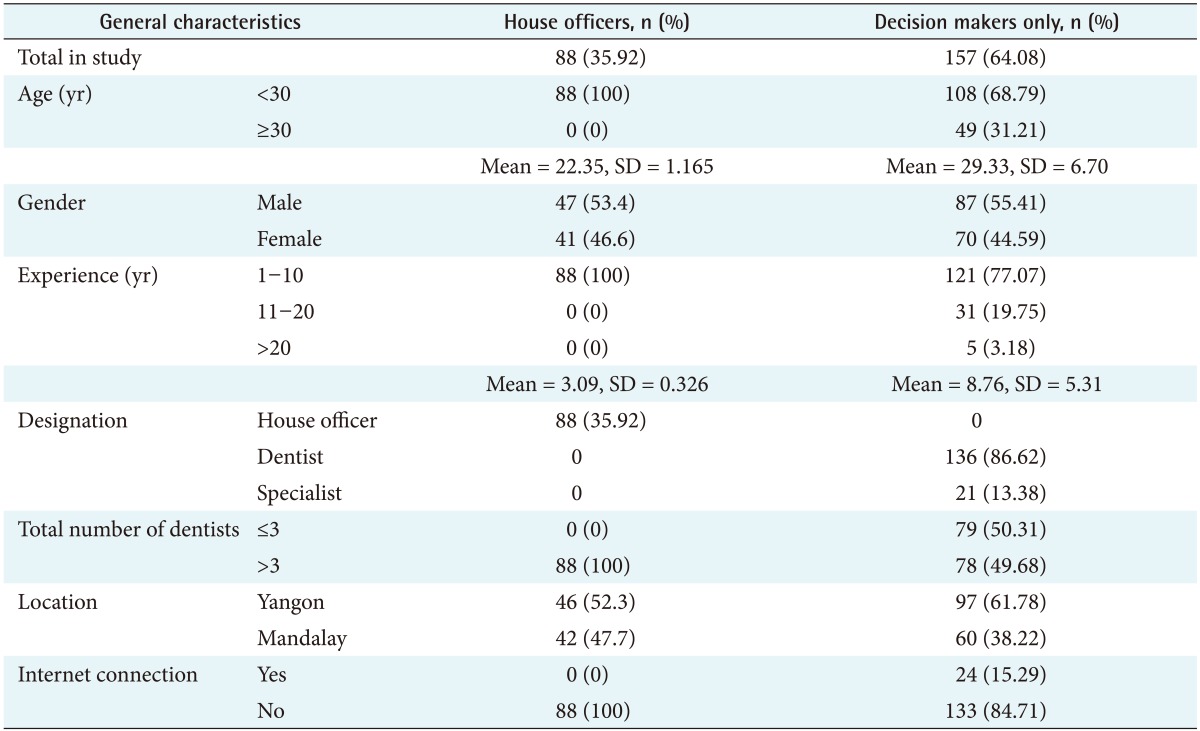
A cross-sectional paper-based survey questionnaire was developed and distributed among dentists who were working at private dental clinics and/or at one of two government teaching dental hospitals, along with house officers who were receiving internship training at the University of Dental Medicine, Yangon and Mandalay. Dental professionals who already had experience with EDR software were excluded from the study. Participants were purposively selected, and interviewers gave them a brief explanation of EDRs before they completed the survey questionnaires. The questionnaire consisted of two parts, with part one completed by all participants in this study. However, part two of the questionnaire was completed only by decision makers at private dental clinics who were responsible for making the decision to switch to an EDR system in their practice. Part one collected information about demographic characteristics and satisfaction with the currently-used paper-based dental records in their clinic. The level of agreement on satisfaction with various aspects of paper-based dental records, such as their perceived usefulness and ease of use, was determined using a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Part two of the questionnaire comprised questions for assessing perceptions of EDRs, including perceived usefulness, ease of use, intention to use them, barriers for implementation, maximum affordable price in their dental clinics, and desirable components of EDR software. This survey questionnaire was constructed based on a previous survey questionnaire developed by Tange and an original technology acceptance model proposed by Davis [
1112]. The technology acceptance model (TAM) is the theory that is used to explain users’ acceptance of new technology. The original technology acceptance model was proposed by Davis in 1989. It is one of the most popular models to evaluate and predict user acceptance of information systems and information technology. In this model, attitudes toward using information technology are influenced by two factors, perceived usefulness and perceived ease of use. There have been many modifications of TAM by including the TAM2 and the unified theory of technology acceptance. Original and modified TAMs have been used extensively in research on health informatics and business research [
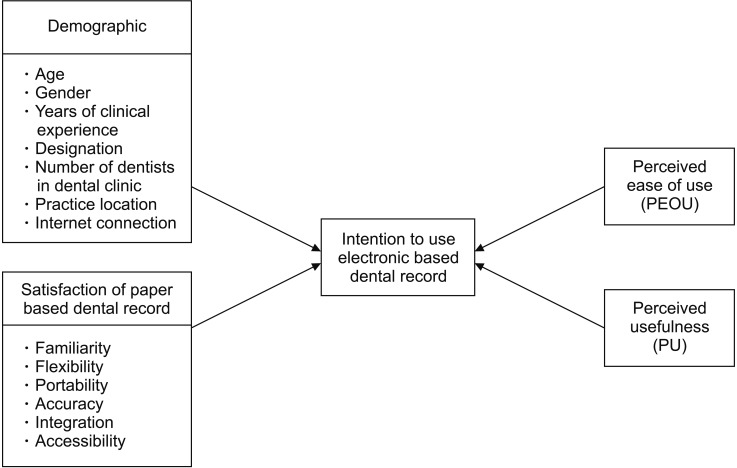
13]. The conceptual framework for the research is shown in
Figure 1. The construction of the research conceptual framework is defined as follows:
‘Perceived usefulness’ means the extent to which an individual believes that using a particular system would increase his or her job performance [14].
‘Perceived ease of use’ refers to the perception of an individual that using the particular system would reduce physical and mental effort [14].
‘Intention to use an electronic dental record system’ refers to a person's motivation to use such a system [14].
‘Barriers to implementation’ are defined as an individual's perception of the factors that prevent the implementation of an EDR system [8].
‘Satisfaction with paper-based dental records’ is defined as the level of an individual's acceptance of the use of paper-based dental records [12].
‘Portability’ refers to the ability to carry a patient's record easily to the point of patient care [12].
‘Availability’ refers to the ability to look the patient's record to check a patient's health history and current health status [12].
‘Flexibility’ means the ability to select the desired words to describe content in the patient's dental records [12].
‘Integration’ can be defined as the ability to combine dental records and medical records or dental records of two or more clinics to give better patient care [12].
‘Familiarity’ refers to the ability of dental professionals to easily and comfortably use patients' dental records [12].
‘Accuracy’ means that a dental professional can record a patient's data such that the record is as close as possible to the true observation [12].
The validity and reliability of the questionnaire was discussed with the thematic paper committee members. Potential participants were asked to read and complete a participant information sheet as well as an informed consent form to ensure voluntary participation. All information and results with personally identifiable information were kept confidential. The study was approved by the Research Ethics Committee of the Faculty of Tropical Medicine, Mahidol University, Thailand. The analyses were performed using SPSS ver. 20 (IBM, Armonk, NY, USA). Cronbach's alpha coefficient was used for the validity and reliability measure of the questionnaire. Descriptive statistics with percentage, mean, and standard deviation were used to report the demographic characteristics of the sampled population, scores of paper-based satisfaction, barriers, choice of maximum affordable price, and perceptions and intention to use an electronic dental record system. Regression analyses were carried out, with the level of statistical significance considered to be 95% (α = 0.05) to identify significant factors influencing the outcomes including total perception and intention to use an electronic dental record system.
IV. Discussion
One of the most important findings of this study was that the majority of dental professionals were satisfied with all of the three strong aspects of paper-based dental records, namely, familiarity, flexibility, and portability. The familiarity aspect received the most positive responses in this survey, which was not surprising as respondents had been using paper-based records since they were in undergraduate dental school. The flexibility of paper-based records was also strongly supported, with most physicians expressing satisfaction because they could choose a variety of words to describe what they wanted to express, which is similar to the findings of Tange [
6]. In this study, most of the respondents were also satisfied with the accuracy of paper-based records, again showing good agreement with the findings of Tange's previous study [
12]. A further crucial finding of the present study was the fact that respondents were unsatisfied with two of the three aspects of paper-based dental records, namely, their accuracy and integration. Inaccuracy may result from the unclear handwriting of dental professionals on paper-based dental records. This also agrees with the results of a previous study conducted in Australia, in which electronic health records were perceived to provide more accurate and more complete information than paper-based dental records [
18]. In addition, almost all of the dental professionals surveyed in the present study wanted to integrate medical records and dental records to improve the quality of patient care in dental clinics. The reason for this finding could be the unreliability of medical histories obtained from patients and dental professionals' wish to prevent undesired events during dental treatment due to compromised medical conditions of patients. Structural integration of medical and dental records is needed to provide comprehensive patient-centered healthcare [
19]. A survey-based study in Canada also revealed that most Canadian dentists wanted to use EDRs to consult with other dental specialists; this agrees with the findings of the current study regarding the intention to integrate records between dental clinics [
20]. However, integration of records between clinics is not easy. As a recent study in Korea showed, there is a lack of health information exchange between external organizations, such as clinics, hospitals, or government organizations due to several complex issues, such as patient's privacy protection, legal requirements, and technological infrastructure problems [
21]. The findings of this study showed that dental professionals were satisfied with only three (familiarity, flexibility, and portability) out of six aspects of paper-based dental records. Therefore, software developers should make serious efforts to improve the familiarity, flexibility, and portability of electronic dental record software in the future. Such efforts are all the more desirable because the adoption of an electronic system is less likely if most dental professionals are more satisfied with the strong aspects of paper-based dental records in comparison with electronic record systems [
12]. This conclusion is also supported by the results of the logistic regression analysis conducted in this study, which showed that user satisfaction was a negative influence on intention to use EDR systems by decision makers (see
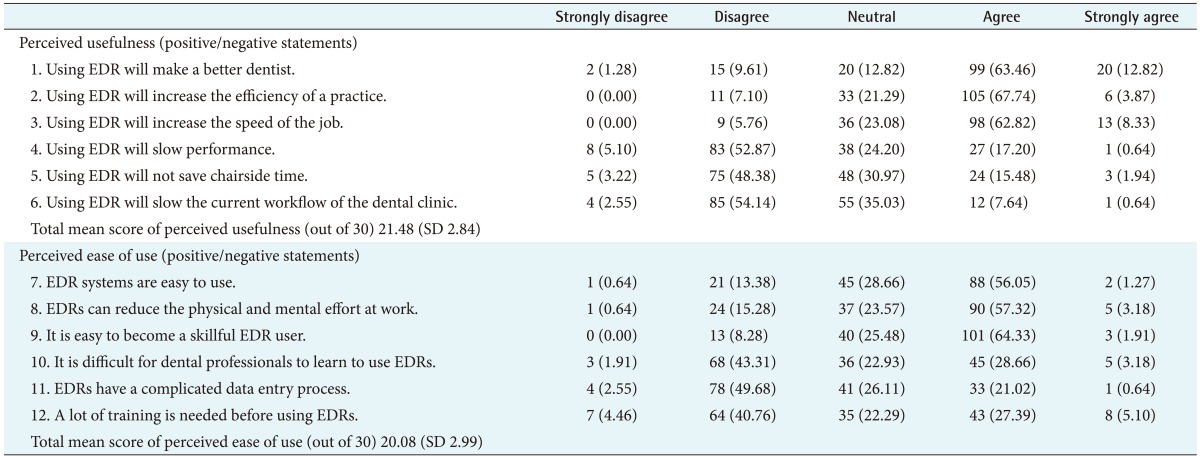
Table 6). A generalized positive perception among decision makers in dental clinics towards electronic patient records was expressed in this survey, as illustrated by the mean total perception score of 41.56 (SD = 4.46) out of 60. This is in agreement with the results of a study conducted at Saudi Arabia Dental College, in which most dental students had a generalized positive perception to the Dentoplus software system 1 year after its implementation at that college [
22]. However, the results of the present study in Myanmar may be over-optimistic, since respondents did not have any experience with electronic dental records, leading to the possibility of their ignoring drawbacks of EDR systems at this time. Furthermore, 86% of decision makers in dental clinics were willing to use EDR software despite a number of barriers being identified. However, this study has revealed the increased potential for future use of an EDR system in dental clinics in Myanmar. This idea is supported by an earlier technology acceptance model proposed by Davis, in which behavioral ‘intention to use’ is one of the preceding factors that can result in the actual use of such a system [
13].
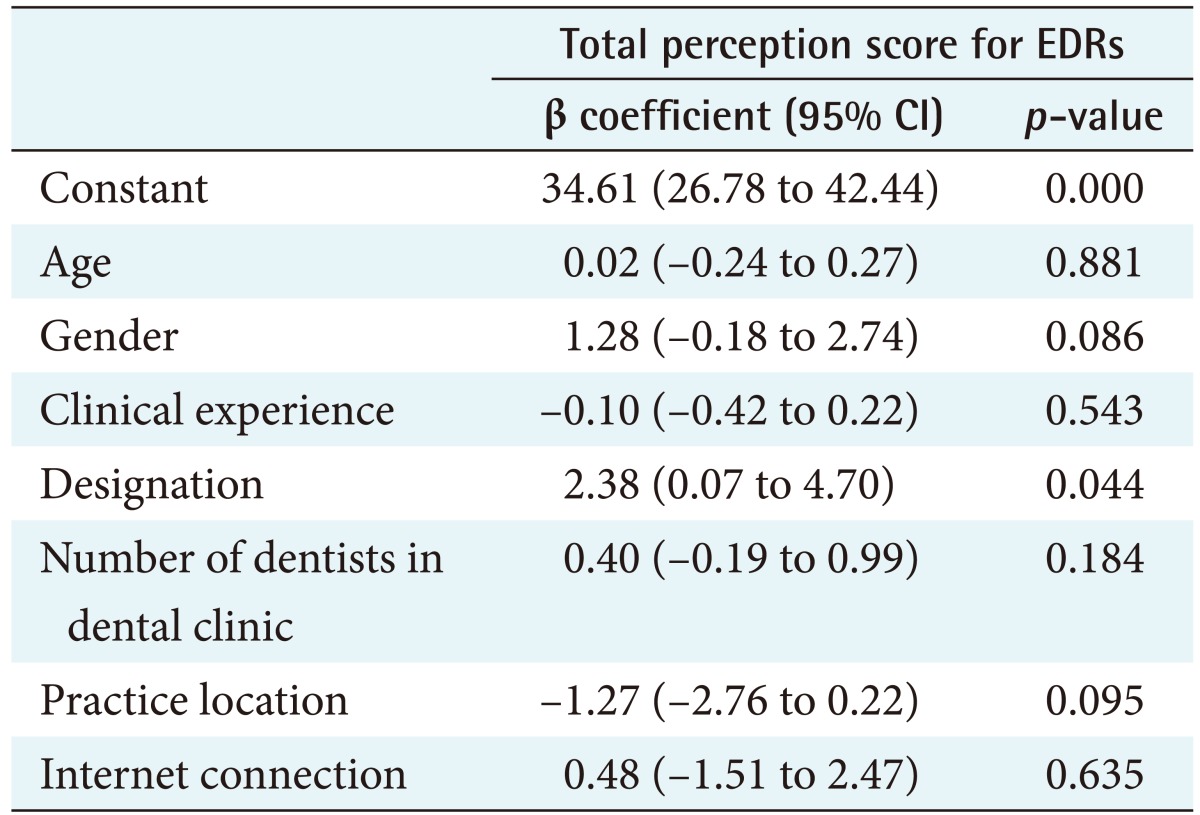
One of the most significant results noted in the multiple regression analysis was that designation was the only influential factor for the total perception score of EDRs by decision makers. This was further confirmed by the higher mean total perception score among specialist dentists (43 out of 60) in contrast with general dentists (41 out of 60) in this study. Generally, specialists are more likely to deal with complex and advanced procedures in dentistry, requiring the assistance of an electronic record system for clinical decision support or advanced analysis of radiographs using software. A previous study conducted in the Netherlands also found that specialists were more motivated to improve the quality of care for their specialized dental treatment [
10]. The total score for perceived ease of use was influenced by clinical experience, the number of dentists in the dental clinic, and the designation of dentists, according to the results of the multiple regression analysis in this study (data not shown). Increased clinic size and the presence of a specialist dentist increased the likelihood of EDR software use in these clinics (data not shown). These findings agree with those of previous studies, in which larger practices and specialist dentists were more likely to use EDRs than smaller practices and general dentists [
1023]. Moreover, additional years of clinical experience with paper-based dental records made the use of EDRs more complicated and difficult for some dentists. Dentists practicing in Yangon division tended to produce higher perceived usefulness scores. This might be related to differences in attitudes towards the performance of advanced technology due to differences in socioeconomic factors between the two divisions. According to the logistic regression analysis results in
Table 6, perceived usefulness and perceived ease of use were the significant determinants of intention to use electronic dental records by decision makers. A recent study also found that the intention to use electronic devices increased with the perception that these devices were effective and convenient to use [
24].
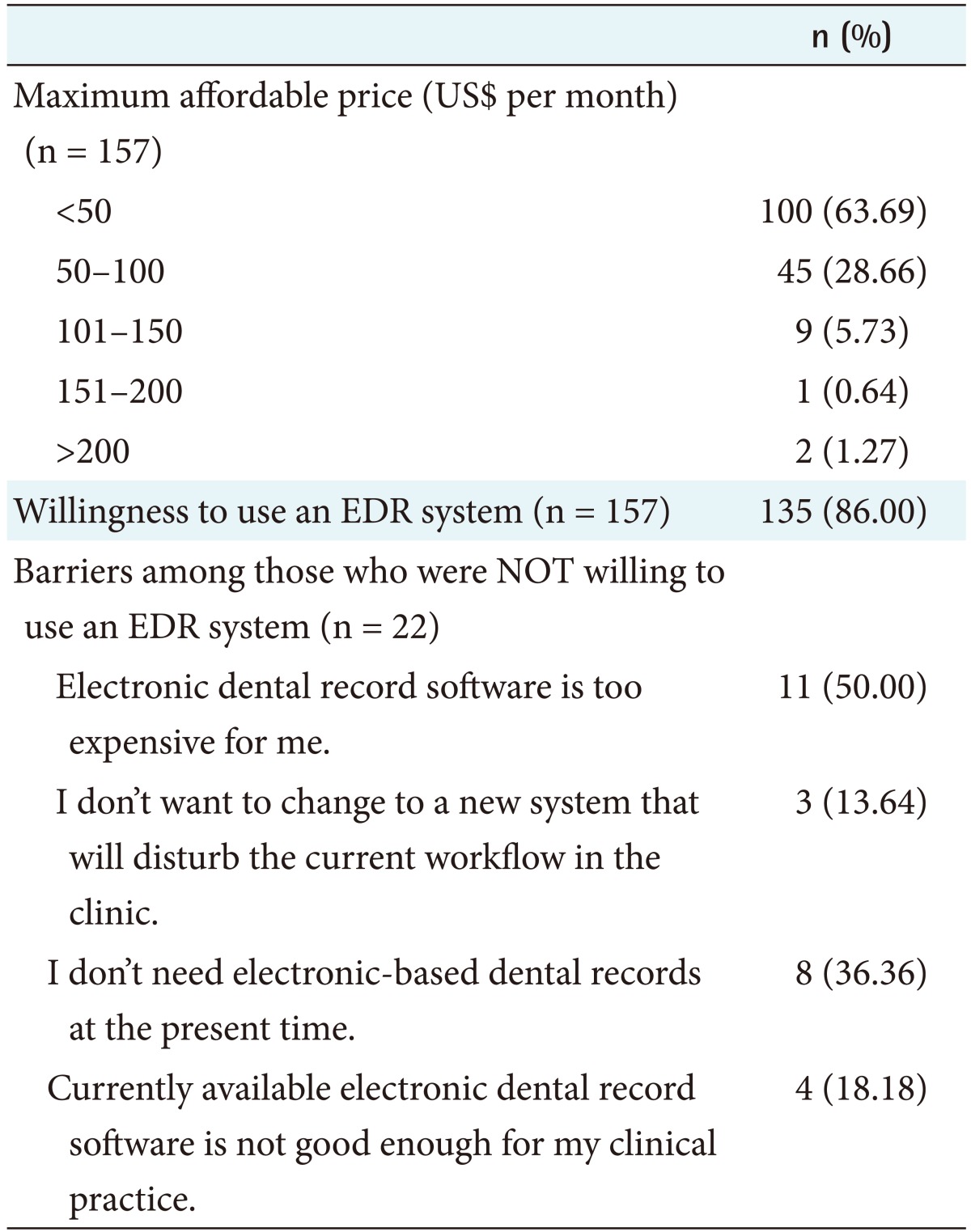
Financial barriers were identified as one of the most important barriers among Myanmar dentists, along with the maximum affordable price of dental software, as shown in
Table 4. This might be influenced by the overall economic situation in Myanmar. Generally, dentists do not want to invest in an electronic record system since the potential benefits of using electronic records are unlikely to cover their investment in software, hardware, and training of personnel in their clinics. Studies conducted among Indian undergraduate dental students, Canadian dentists, and US dentists also concluded that financial barriers were one of the major obstacles for the implementation of digital technology in dental clinics [
22025]. A feasibility assessment study of Electronic Medical Record at Marie Stopes International's Clinics in Myanmar found that some of the major concerns of healthcare providers were extra workload, training requirements, accessibility, confidentiality of data, as well as the availability of technical support and infrastructure. They did not worry about financial concerns, unlike the participants in the present study, because they could get private funding from a non-government organization for implementation of technology in their workplace [
3]. Since most dental professionals in Myanmar did not use the Internet with either laptop or desktop computers in their clinics, they were less likely to buy a Wi-Fi package for their practice. Wi-Fi connection was available in just 10% of dental professionals' practice areas and 15% of dental clinic owners' practice areas, which may contribute to limiting the effective implementation of an EDR system in the future.
In conclusion, this study found that dental professionals were only satisfied with three out of six aspects regarding the use of paper-based dental records, despite this system being in use for over 50 years in Myanmar. Furthermore, most dentists surveyed expressed intention to use an electronic record system, even if they could not afford to implement it in their clinics at the present time due to financial barriers. To draw up a step-by-step strategy for the implementation of an EDR system in Myanmar, there should be both a short-term and a long-term plan. The first and most important step in moving towards an EDR system should be proper record keeping and improvement of the structure and organization of the currently paper-based dental record system, especially in private dental clinics. Utilization of appropriate open-source EDR software in private dental clinics is strongly recommended to overcome the financial barriers to its implementation. For the long-term, we recommend that additional education should be provided to healthcare professionals. For example, a biomedical and health informatics element could be introduced in undergraduate dental courses in Myanmar's two medical schools to prepare students for the use of platforms using advanced technology which could support their work in the future.