Scenario-Based Assessment of User Needs for Point-of-Care Robots
Article information
Abstract
Objectives
This study aimed to derive specific user requirements and barriers in a real medical environment to define the essential elements and functions of two types of point-of-care (POC) robot: a telepresence robot as a tool for teleconsultation, and a bedside robot to provide emotional care for patients.
Methods
An analysis of user requirements was conducted; user needs were gathered and identified, and detailed, realistic scenarios were created. The prototype robots were demonstrated in physical environments for envisioning and evaluation. In all, three nurses and three clinicians participated as evaluators to observe the demonstrations and evaluate the robot systems. The evaluators were given a brief explanation of each scene and the robots' functionality. Four major functions of the teleconsultation robot were defined and tested in the demonstration. In addition, four major functions of the bedside robot were evaluated.
Results
Among the desired functions for a teleconsultation robot, medical information delivery and communication had high priority. For a bedside robot, patient support, patient monitoring, and healthcare provider support were the desired functions. The evaluators reported that the teleconsultation robot can increase support from and access to specialists and resources. They mentioned that the bedside robot can improve the quality of hospital life. Problems identified in the demonstration were those of space conflict, communication errors, and safety issues.
Conclusions
Incorporating this technology into healthcare services will enhance communication and teamwork skills across distances and thereby facilitate teamwork. However, repeated tests will be needed to evaluate and ensure improved performance.
I. Introduction
Telehealth is defined as the use of telecommunications to provide health information and care across distance [1]. It may improve access to specialists by redistributing expertise in given care contexts virtually [2]. The adoption of telehealth technologies greatly reduces location as a barrier to accessing high-quality treatment and care, opening up new opportunities for healthcare providers to engage with patients and other professionals across distances. In Korea, the concentration of large hospitals in urban areas causes many problems, such as inequity of access to health facilities and services, missing optimal time of treatment, and increasing health care expenditures due to unnecessary transfers and repeated laboratory tests [34]. Teleconsultation using telehealth technologies could solve these problems by facilitating the exchange of medical information to assist diagnosis and treatment at a distance.
In prior studies, telemedicine or teleconsultation using videoconferencing has been shown to improve access and the quality of clinical care available to rural patients. Also, it can lead to lower costs through the reduction of unnecessary transfers [56789]. Furthermore, studies have reported that professional development opportunities and support from specialists may help improve rural medical workforce recruitment and retention [1011]. However, most teleconsultations are asynchronously conducted, and response time is an important factor in facilitating rapid diagnosis and finding appropriate treatments for diseases in telemedicine and teleconsultation. That is, a lack of extemporaneity is a limitation of care [29].
In addition, the main users of these systems are healthcare providers, not patients. Patients admitted to hospitals and their unformal caregivers may be passive due to a lack of information, and they tend to become dependent on their healthcare providers. Furthermore, many inpatients feel anxiety and fear regarding upcoming treatments, but healthcare providers cannot allot enough time for emotional care. Point-of-care (POC) refers to situations in which healthcare providers deliver health services to patients at the time of care and not asynchronously [12]. This approach aims to capture the patient's healthcare needs and deliver proper treatment and care in a timely manner. Bedside terminals are currently used in point-of-care settings, generally to provide medical content or web browsing services; however, they do not sufficiently support emotional care for patients [13]. In the holistic view of healthcare, emotional needs are considered inextricable from physical and psychological needs. For this reason, we are currently developing two types of POC robots: a telepresence robot as a tool for teleconsultation, and a bedside robot for emotional care of patients.
It is critical to understand the factors that may increase acceptance and adoption of healthcare robots so that robots can be designed in such a way that they will be more likely to be adopted [1415]. Therefore, we conducted scenario-based demonstrations to assess what users need from POC robots and to define the functions of the robots prior to system development. In this paper, we will address methodological aspects related to the development of these POC robots for healthcare and will discuss the results of implementing those approaches. The objective of this study was to derive specific user requirements and barriers in real medical environments.
II. Methods
Scenario-based assessment is an efficient method to understand the hospital environment in relation to the end needs of users, including healthcare providers, patients, and informal caregivers. We implemented an analysis of user requirements, which was a simple process encompassing four elements; (1) information gathering, (2) user needs identification. (3) envisioning and evaluation, and (4) requirements specification [16].
1. Gathering Information on the User's Context
User surveys and interviews were conducted to determine the needs of users, current work practices, and issues that need to be addressed. We also conducted field observations to gain significant information concerning the users' contexts, the equipment in use, and the place of work. To gain awareness of the drawbacks of traditional consultation through videoconferencing, we interviewed clinicians and nurses and observed the service from the user's perspective. Also, a number of hospitals have installed bedside terminals for patients; to compare existing bedside terminals, we visited hospitals that provide similar services.
2. User Needs Identification
We developed scenarios and use cases to give detailed, realistic examples of how users may carry out their tasks in specific contexts using robots. A simulated patient was defined, and the medical records of the patient were created. The developed scenario consisted of three parts, each with 3 to 4 scenes, across which the expected functions of the POC robot were mapped.
3. Envisioning and Evaluation through Scenario Simulation
Once the intended functionalities had been defined, it was important to develop a prototype to illustrate them. Feedback from evaluators could then be obtained to validate and refine the user needs. Clinicians developed, reviewed, revised, and completed the scenarios for the demonstrations. A total of 9 researchers (2 clinicians, 4 clinical nurses, and 3 system developers) were involved.
The robots tested in the demonstrations were not intended to be perfect. Imperfections such as technical errors and delays of operation are inevitable. To help reflect this reality, user responses could be assessed in both ideal and near-real cases throughout the scenario-based demonstrations. In all, 3 nurses and 3 clinicians participated as evaluators to observe the demonstrations and evaluate the robot system after they had been given a brief explanation of each scene and the robots' functions. It is necessary to conduct demonstrations of POC robots in physical environments that simulate the conditions of the work situation at a high level of realism [13]. Our scenario-based demonstrations took place in a simulation center with an emergency department, an operation room, and general wards. All the demonstrations were filmed for further evaluation.
4. Specification of Requirements
After the scenario-based demonstrations, the evaluators completed a report form, which was used to evaluate the robots and to measure their usability. The usability scale had 8 items scored on a 100-point scale. Further, unstructured interviews were conducted. Examples of prompt questions used to guide the interview included the following: “In the POC robot systems to be developed, what are the most important functions to be included?”, “How does the POC robot system facilitate or obstruct patients' treatment and care when the system is integrated into a real medical environment?”.
III. Results
1. Gathering Information on the User's Context and User Needs Identification
1) Teleconsultation robot
Ninety participants including 39 physicians and 51 nurses were surveyed. Among the desired functional requirements for a teleconsultation robot, medical information delivery, a wireless system, and screen sharing had the highest priority in that order. The internal medicine and surgical wards, operating room, and outpatient clinic revealed greater need for such a system.
The major themes derived from the interviews included major functions, usability, expected effects, and anticipated issues. The subthemes of the major functions were communication, visual, and data-sharing functions. The subthemes of usability were movability, the form of the device, and convenience for users. The major expected effects included ‘prevention of delays in treatment’ and ‘assistance in decision making on transferring a patient’. The major anticipated issues included ‘anxiety about the robot’, ‘judgment error’, and ‘limitations in use at some divisions’.
2) Bedside robot
In all, 198 participants including 108 patients, 39 physicians, and 51 nurses were surveyed. The desired function requirements for a bedside robot included prediction of patient's events, call bells, and support for physician's rounds.
The major themes derived from the interviews included the major functions, usability, and anticipated issues. The subthemes of the major functions were patient support, patient monitoring, and healthcare provider support. The subthemes of the major functions were patient support, patient monitoring, and healthcare provider support. The subthemes of usability were the form and movement of the robot as well as methods of fixation. The subthemes of anticipated issues included ‘increased workload of healthcare providers’ and ‘regard only as an amusement tool’.
2. Development of Scenarios for Demonstrations
According to the information gathered through the surveys and interviews, four major functions of the teleconsultation robot were defined and tested in scenario-based demonstrations: (1) image acquisition using a super-wide-angle camera and a high-resolution camera, (2) image transmission and display, (3) remote control of the robot's arms, and (4) mobility of the robot. Similarly, four major functions of the bedside robot were also evaluated: (1) bidirectional video system, (2) support system of doctor counseling, (3) voice recognition, and (4) ability to recognize non-verbal expressions of the patient. The functions of both types of robots were placed in the appropriate scenarios for them to be tested (Table 1). To evaluate these functions, prototypes of the POC robot were developed. The technical specifications of each robot are shown in Table 2.

Summary of demonstrated scenes and required functionalities

Technical specification of the point-of-care robots
The simulated patient was a 52-year-old female admitted to an emergency department for headache and memory impairment. Patient data for this simulated patient was derived from real patient data. Clinicians reviewed and revised draft scenarios in which the specific situation, including place and time, was defined, and each scene was explained in detail. Hospital S was defined as an on-site hospital requesting teleconsultation, while hospital M was an off-site hospital providing teleconsultation. Examples of final scenarios are shown in Tables 3, 4, 5.

Scenario of teleconsultation in an emergency department
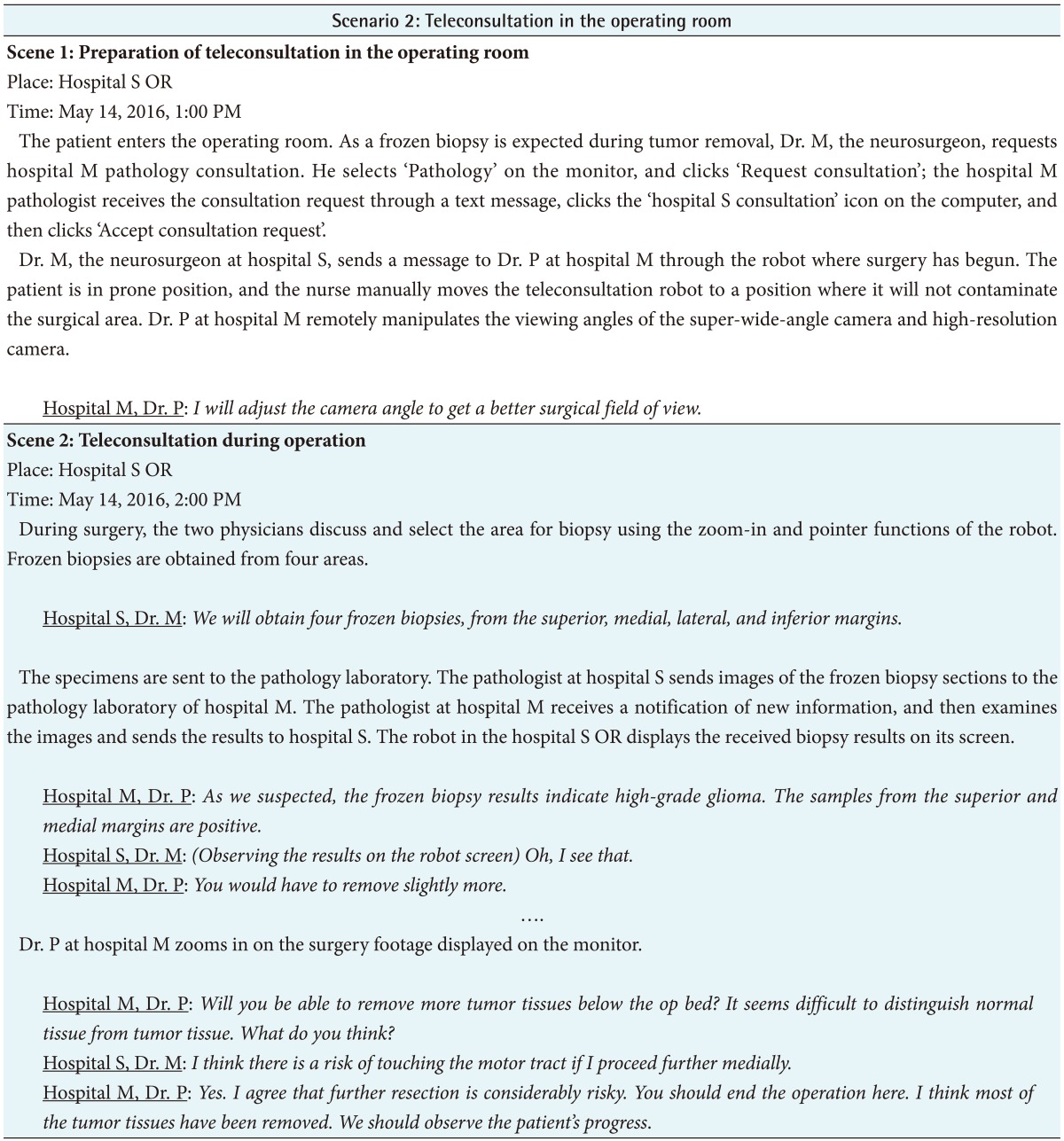
Scenario of teleconsultation in an operating room
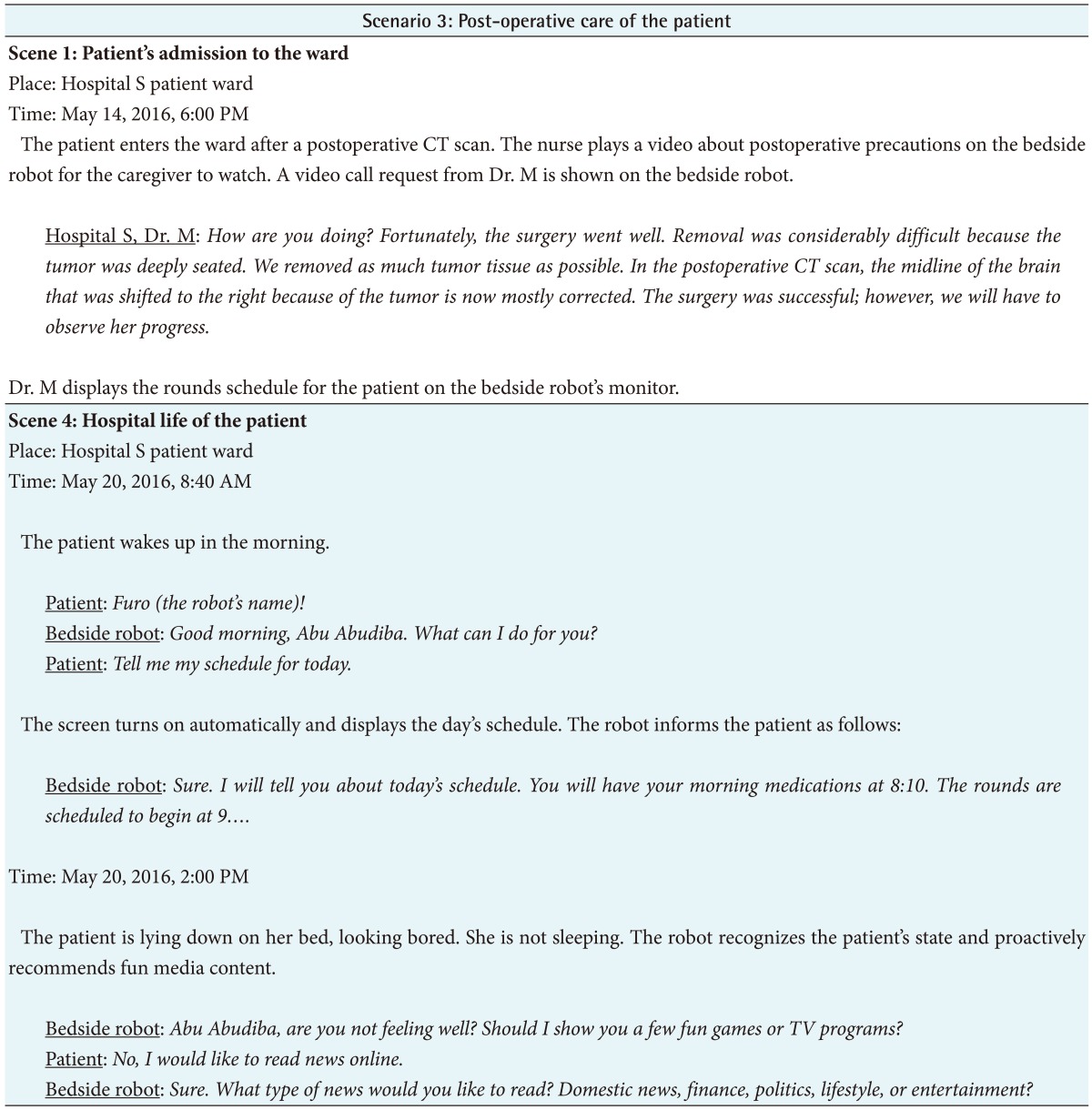
Scenario of post-operative care of the patient
3. Envisioning and Evaluating the POC Robot System and Requirement Specification
A total of four research assistants took roles as two clinicians, a nurse, and a family caregiver (Figure 1). The upper left part of Figure 1 shows the evaluation of image acquisition using a super-wide angle camera, and the upper right part shows the function of the mobility of the robots. The lower left part of Figure 1 shows communication using a bidirectional video system. In the lower right part, the patient and her family caregiver watch educational video contents.

Scenario-based demonstrations of the point-of-care robots.
The scores for the usability of the POC robots are shown in Table 6. After the demonstrations, the participants, including scenario developers, research assistants, and observers discussed the results informally. The evaluators reported that both types of POC robots were acceptable, and the problems identified based on the demonstrations were those of space conflict, communication errors, and safety issues (Table 7).
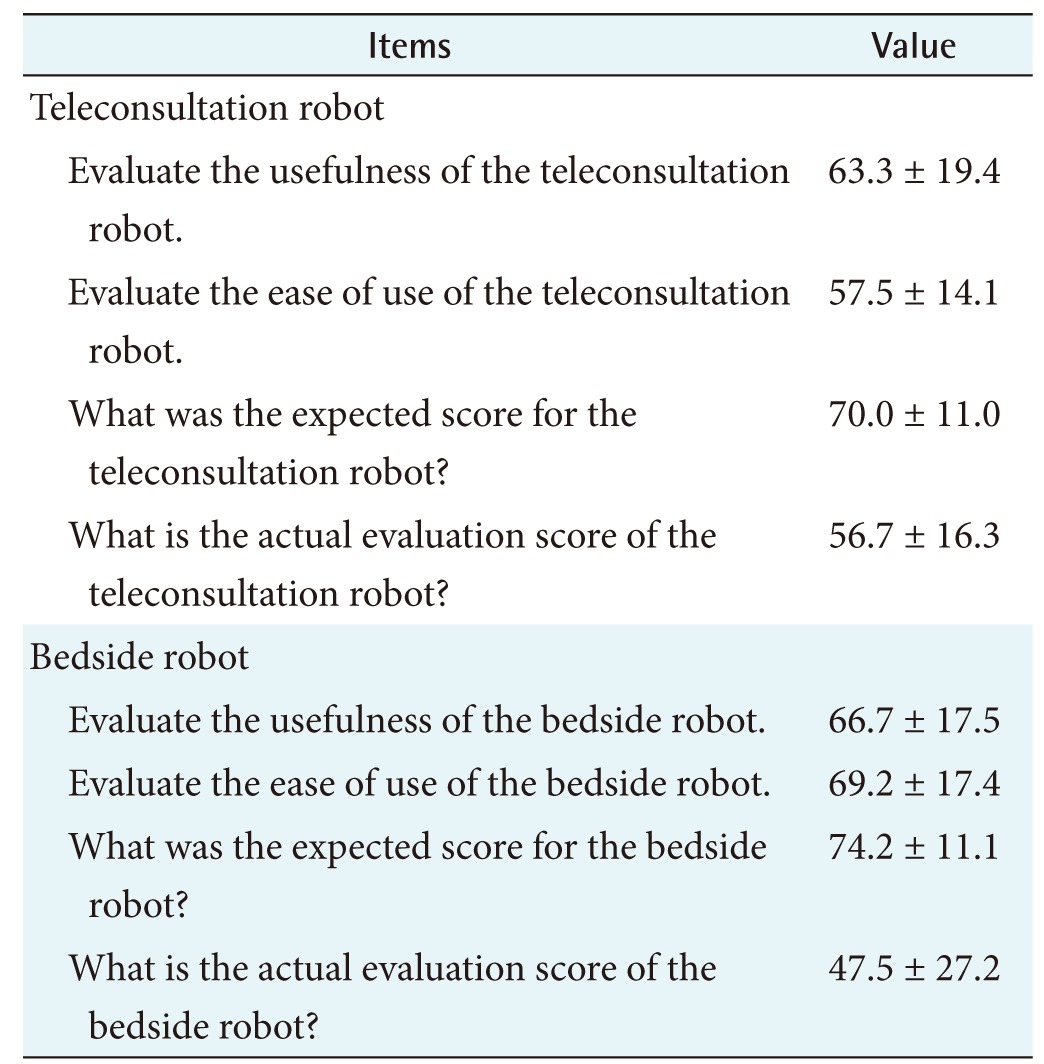
Usability of the point-of-care robot after scenario-based assessment (n = 6)
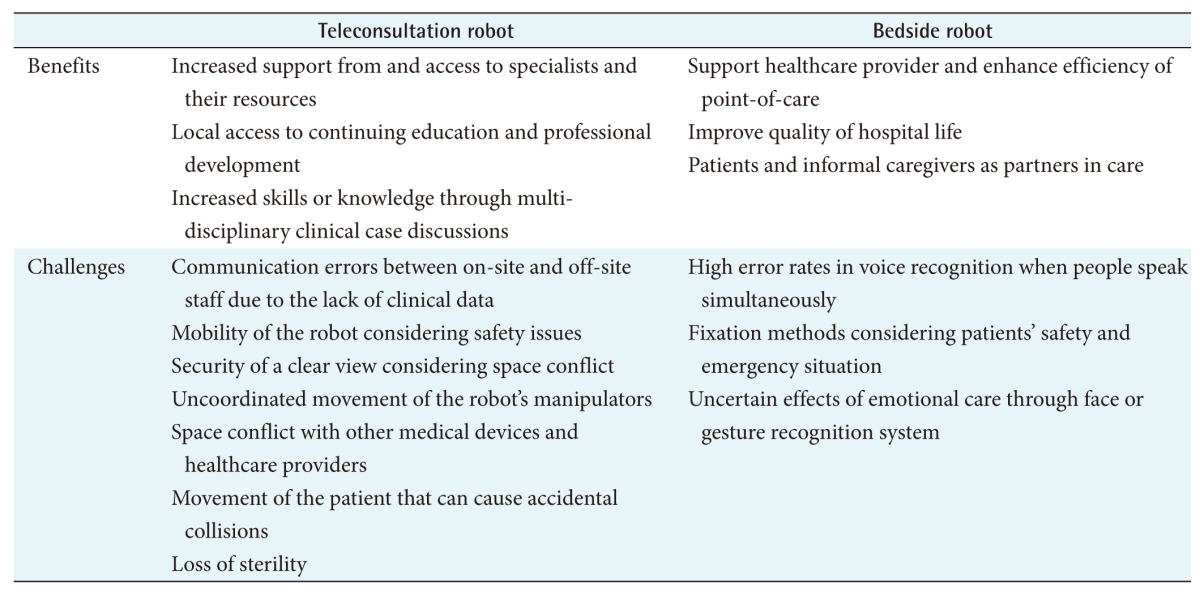
Expected benefits and challenges of the point-of-care robot
IV. Discussion
Evaluating prototypes in an actual hospital is not allowed due to patient safety and privacy issues. Hence, system developers often face difficulties in representing user requirements in an appropriate form [16]. In this study, the POC robot systems were assessed through user requirement analysis based on scenario-based demonstrations. This allowed the evaluation of multiple functions and the identification of use strategies before their actual implementation in the medical field.
We found that it was feasible to use the teleconsultation robot for difficult cases. Consultations were conducted in real time, and it was possible to request additional information and assess patients directly. This is important because the quality of treatment and care are strongly influenced by proper timing [29]. The teleconsultation robot has two types of cameras for image acquisition, a super-wide-angle camera and a high-resolution camera. This is essential for participation in distant events; it gives distant healthcare providers a closer look at not only the patient's critical areas but also the surrounding environment for consultation and educational purposes.
Several evaluators mentioned that another benefit of using the teleconsultation robot was that it allowed continual learning and accumulation of experience under the instruction of specialists. Wang et al. [9] pointed out that hospitals that provide consultation and education should be more proactive in regularly scheduling online teaching rounds, consultations on difficult cases, and other types of diversified tele-education activities to provide access to ongoing medical, educational, and training support.
One of the drawbacks of the implementation was space conflict with other medical devices and healthcare providers. When robots are used in operating rooms it is crucial to maintain sterility and patient safety, meaning that the robots must have bigger, heavier bodies to allow stable fixation. On the other hand, in general wards, a slim form would be appropriate to aid functions such as person tracking or autonomous navigation function. Accordingly, we are considering developing two different types of teleconsultation robots separately for use in operating rooms and general wards.
In these assessments, the physicians used PC-based programs to provide consultation; however, in real-world medical environments, it is not easy to sit in front of a PC in all situations. In this respect, it is important for health professionals to use tablet PCs or smartphones in teleconsultations. A language translation function should also be considered to allow teleconsultation with practitioners in other countries. Additional use of peripherals, such as electronic stethoscopes and radio frequency identification (RFID) can be considered as well.
Various types of bedside terminals are already in use, and bedside robots also need differentiation in the point-of-care aspect. Healthcare providers can share test results or view diagnostic images with a patient during staff rounds so that patients and informal caregivers can serve as partners in care. The patient can record the staff rounds and reproduce them as many times as desired so that physicians and nurses do not need to repeat the same explanations. Voice commands using activation phrases enable patients with limited physical ability to control the robot without touch, turning it on and off, calling their nurse, or playing educational videos or entertainment options. In this way the bedside robot is expected to play a major role in raising patient satisfaction and enhancing healthcare productivity.
Among the various functions evaluated, a major one was care through face or gesture recognition. The robot not only operates passively according to the user's commands but also starts conversations based on recognition of the patient's condition. When the patient wakes up, the bedside robot recognizes this and wishes the patient good morning. Then, based on the scheduled surgery or procedure, the robot recommends educational content, for instance. Existing bedside terminals are designed to perform simple tasks or to be used purely for entertainment; however, as robot capability increases, personal use will encompass a greater variety of tasks and more complex social functions [13]. The social capability of the robot may indeed critically influence its acceptance, as variables such as social intelligence, emotion expression, and nonverbal social cues may influence user expectations about the robot's social capability [17]. Incorporating this function into bedside robots will not only improve patients' quality of hospital life but also support POC service provision.
In the scenario-based assessment, evaluators indicated errors in voice recognition when more than one user spoke at the same time. In the active state, surrounding noise should be technically filtered, and only the voice of the nearest user should be recognized. Evaluators also emphasized that the method of fixation is very important, because the robot should be removable easily and quickly in an emergency.
The present study had some limitations. First, subjective assessments were obtained through self-report methods. Therefore, an objective scale should be used for measurement to improve validity in repeated evaluations. Second, the results may have been biased because of the small number of evaluators. Third, the prototypes of the robots were immature; hence, further research must be undertaken that reevaluate and improve the robots.
While there remain challenges, incorporating this technology into healthcare services will enhance information-sharing across distances and thus will facilitate teamwork. Repeated evaluations will be needed to ensure improvement in performance.
Acknowledgments
This research supported by the Ministry of Trade, Industry & Energy (MOTIE) of Korea under Industrial Technology Innovation Program (No. 10063098, Telepresence robot system development for the support of point-of-care service associated with ICT technology).
The authors greatly appreciate Professor Sukwha Kim and Professor Hyoun-Joong Kong for valuable guidance on this project. We would also like to thank Meihua Piao, Jisan Lee, Ahjung Byun, Hyeongju Ryu, HyunJin Joo, EunJin Hwang, and Ha Min Sung for support of this study.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.