A Three-Year Autoregressive Cross-Lagged Panel Analysis on Nicotine Dependence and Average Smoking
Article information
Abstract
Objectives
Previous studies have been limited to the use of cross sectional data to identify the relationships between nicotine dependence and smoking. Therefore, it is difficult to determine a causal direction between the two variables. The purposes of this study were to 1) test whether nicotine dependence or average smoking was a more influential factor in smoking cessation; and 2) propose effective ways to quit smoking as determined by the causal relations identified.
Methods
This study used a panel dataset from the central computerized management systems of community-based smoking cessation programs in Korea. Data were stored from July 16, 2005 to July 15, 2008. 711,862 smokers were registered and re-registered for the programs during the period. 860 of those who were retained in the programs for three years were finally included in the dataset. To measure nicotine dependence, this study used a revised Fagerström Test for Nicotine Dependence. To examine the relationship between nicotine dependence and average smoking, an autoregressive cross-lagged model was explored in the study.
Results
The results indicate that 1) nicotine dependence and average smoking were stable over time; 2) the impact of nicotine dependence on average smoking was significant and vice versa; and 3) the impact of average smoking on nicotine dependence is greater than the impact of nicotine dependence on average smoking.
Conclusions
These results support the existing data obtained from previous research. Collectively, reducing the amount of smoking in order to decrease nicotine dependence is important for evidence-based policy making for smoking cessation.
I. Introduction
In Korea, the highest point in the country's adult smoking rate was in 1980 (male, 63.5%; female, 12.6%); currently, (as of June 2011), 39.0% of adult males and 1.8% of adult females smoke. The decrease in smoking prevalence can be attributed to the combined influences of the national health promotion law legislated in 1995 and the increased cost of cigarettes. Specifically, in December 2004, powerful non-smoking policies and supports for smoking cessation were enacted in the nation including prohibited non-smoking areas, smoking cessation clinics in community health centers, telephone counseling for smoking cessation and non-smoking campaigns for public and health education.
Since July 21, 2011, the Ministry of Health and Welfare (MOHW) of Korea has been planning to accelerate implementation of the national comprehensive policy planning which includes the price and non-price policy to drastically reduce the high prevalence of smoking as compared with the Organization for Economic Co-operation and Development (OECD) countries.
While smokers recognize that the habit is injurious to health, smoking cessation is difficult because of nicotine addiction contained in cigarettes [1-4]. Nicotine dependence represents the degree of addiction for smoking, and World Health Organization (WHO) reports the concept that smoking is a disease; therefore, it needs a treatment for nicotine addiction. For this reason, previous research has been conducted to study the relationships between nicotine dependence and smoking. For example, studies have explained that smoking in nicotine-dependent women is less than nicotine-dependent men [3,5]. Rosenbaum and O'Shea [6] also reported that the amount of smoking increases growing nicotine dependence and nicotine-dependent smokers are highly likely to fail when they tried to quit smoking because of withdrawal symptoms. Therefore, nicotine dependence is an important influencing factor in successful smoking cessation.
Rigotti [7] reported that the causes of smoking and nicotine dependence are related. Carlson et al. [8], for example, demonstrated that predictors of successful smoking cessation were the amount of smoking and nicotine dependence. Based on collective results, nicotine replacement therapy emerges as a "help quit smoking" as well as reduces the amount of smoking [9]. Levshin et al. [10] reported that there were several factors predictive of successful smoking cessation including the number of attempts for quitting smoking: the amount of daily smoking, nicotine dependence, and motivation for smoking cessation.
A study conducted by Lee and Seo [11] indicated that the number of cigarettes a day and nicotine dependence yield to low to successfully quitting smokers. Suh et al. [12] also demonstrated that the number of cigarettes a day was a significantly influential factor in quitting smoking for six months (p < 0.05). This study also reported that nicotine dependence was related to only short-term smoking cessation, not long-term maintenance. Song et al. [13] analyzed nicotine dependence of registrants for the smoking cessation programs conducted by community health centers and reported: as nicotine dependence is lower, the success rate of smoking cessation for six months is higher for both new registrants and re-enrollment registrants.
Lessov-Schlaggar et al. [14] supported previous research results [15-17] by adding evidence, through a study employing youth nicotine dependence and the trajectory of smoking, that youth smoking was also related to nicotine dependence. Song et al. [4] reported there were individual differences in the trajectory of nicotine dependence; they also reported that successful experience for smoking cessation reduced nicotine dependence. A recent study [18] also demonstrated that nicotine dependence and the number of cigarettes a day were related to the first smoking age, a total smoking period, drinking, body mass index (BMI), and residential area.
In summary, the majority of previous studies have been limited to the sole use of cross sectional data to identify the relationships between nicotine dependence and smoking. Therefore, with analyses conducted at one selected time point, it is difficult to test and determine a causal direction between the two variables. This study used a panel dataset which contains information regarding attempts for quitting smoking accumulated for three years. The purposes of this study were to 1) test whether nicotine dependence or average smoking was a more influential factor in smoking cessation; and 2) propose effective ways to quit smoking as determined by the causal relations identified.
II. Methods
1. Data Collection
This study used a three-year panel dataset obtained from the central computerized management systems for the smoking cessation programs of the community health centers in the nation. Data were stored from July 16, 2005 until July 15, 2008. 711,862 smokers were registered and re-registered for the programs for the period. 860 of those who were retained for three years in the programs were finally included in the dataset. For the study, success in smoking cessation means smokers did not smoke cigarettes for the past consecutive six months. The rate of success in smoking cessation each year is as follows: 32.7% (1st), 29.7% (2nd), 12.9% (3rd). The majority of the smokers were men (n = 800, 93%). Average age of the smokers was 49.2 years (standard deviation = 12.8 years). About 90% (n = 770) had health insurance. Half (n = 369) lived in smaller cities (Table 1). The reliability of the variables such as nicotine dependence and average smoking, which was measured each year for the three-year period of the study, showed high internal consistency (Cronbach's α = 0.780 and 0.788, respectively).
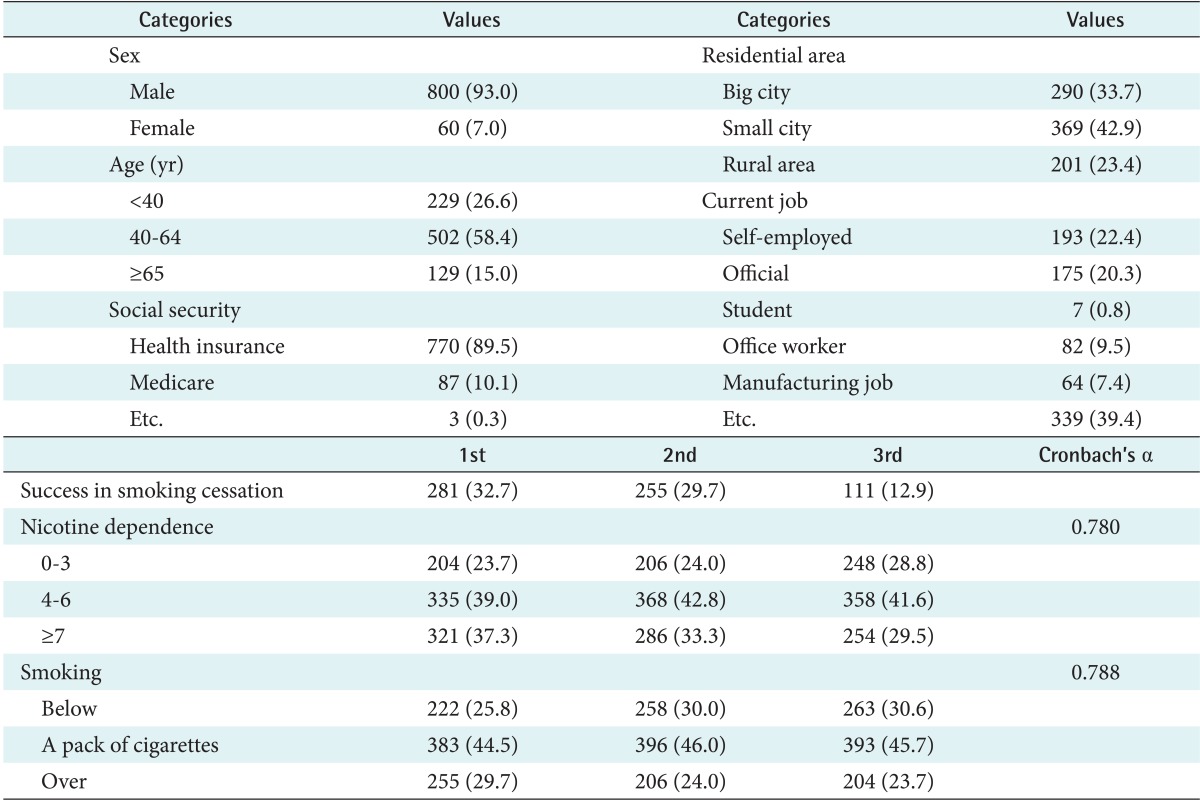
General characteristics (n = 860)
2. Study Variables
To measure nicotine dependence, a revised Fagerström Test for Nicotine Dependence (FTND) was used, which is currently in wide use on a global level [18,19]. The FTND is consisted of the following six items: 1) 'How many cigarettes do you smoke a day?' (0-10, score 0; 11-20, score 1; 21-30, score 2; >31, score 3); 2) 'How soon after you wake up do you smoke your first cigarette?' (≤5 minutes, score 3; 6-30 minutes, score 2; 31-60 minutes, score 1; >60 minutes, score 0); 3) 'Do you find it difficult to refrain from smoking in places where it is forbidden?' (yes, score 1; no, score 0); 4) 'Do you smoke if you are so ill that you are in bed most of the day?' (yes, score 1; no, score 0); 5) 'Do you smoke more frequently during the first hours of waking than the rest of the day?' (yes, score 1; no, score 0); and 6) 'Which cigarette would you hate most to give up?' (morning cigarette, score 1; other cigarette, score 0). In scoring the revised FTND, the items are summed to yield a total score of 0 (very low) to 10 (very high) [19]. The community health centers in Korea also used this questionnaire to measure nicotine dependence of smokers [4,18].
In the study, average smoking was operationalizing as the number of cigarettes smoked a day for the entire smoking period until the smokers visited the smoking cessation clinic in the community health centers.
3. Statistical Analysis
To examine the longitudinal relationships between nicotine dependence and smoking, an autoregressive cross-lagged (ARCL) model was explored. The core of the ARCL is that the value at the time of [t] is explained by the value at the time of the previous point, [t-1] [20,21]. In order to explore the ARCL model, the order of analyses should be followed by homogeneity of measurements, paths, and error covariance.
Homogeneity means that "statistical properties of any one part of an overall dataset are the same as any other part" [22,23]. Homogeneity of measurements is conducted to test whether the concept is measured at each time point for a longitudinal study or measuring the changes on the concept over time. Therefore, factor loadings of the same questions (study variables) should be constrained equally [21]. Because this study employed only one observed variable, homogeneity of measurements was not examined.
Homogeneity of paths is conducted to test the regression coefficients for each observed variable is stable over time. It can be tested by comparing if the impact of the variable (regression coefficient) at the time of [t-1] on the variable at the time of [t] is same with the impact of the variable (regression coefficient) at the time of [t] on the variable at the time of [t+1]. The regression coefficient can be labeled as stability coefficient [21].
To test homogeneity of error covariance is to equally constrain covariance between the errors of the variables. In order to evaluate the goodness-of-fit, χ2 tests and the goodness-of-fit indices were considered. Among the various fit indices, incremental fit indices such as Comparative Fit Index (CFI), Normed Fit Index (NFI), Tucker-Lewis Index (TLI), and absolute indices such as Goodness Fir Index (GFI), Root Mean Square Error of Approximation (RMSEA) were used for the study [24-26].
In general, if the values of incremental fit indices such as the CFI are larger than 0.9, it means that the model fit is good [24,25]. The GFI has a value between 0 and 1, and the value should be greater than 0.9 for a model that fits well. The RMSEA was developed to correct the issue of statistics arising from χ2 tests which include many observed variables. The value of RMSEA should be less than 0.05 for a model that fits well. Values of 0.06 to 0.08 indicate mediocre fit, and values greater than 0.1 indicate poor fit [25-28].
For the analyses of this study, SPSS ver. 19.0 was used for descriptive statistics and average analysis. To analyze the ARCL model, AMOS ver. 20.0 (IBM, New York, USA) for the structural equation modeling was employed.
4. Study Design
The research questions (RQ) of this study are as follows:
RQ 1: Is nicotine dependence stable over the time period?
RQ 2: Is average smoking stable over the time period?
RQ 3: Is the impact of nicotine dependence on average smoking significant?
RQ 4: Is the impact of average smoking on nicotine dependence significant?
The ARCL model was employed to test the above research questions (Figure 1).

Autoregressive cross-lagged model of nicotine dependence and the average smoking.
III. Results
1. Descriptive Statistics and Correlation
Nicotine dependence and average smoking over the time period are described in Table 2. The value of skewness and kurtosis of nicotine dependence and average smoking supported the assumption of normal distribution of the data; the absolute value of skewness is less than 3, and the absolute value of kurtosis is less than 10 [29]. Therefore, there was no statistical problem in testing the ARCL model of structural equation modeling. Because structural equation models assume multivariate normal distribution, analyses were conducted under the assumption that observed variables are normally distributed.
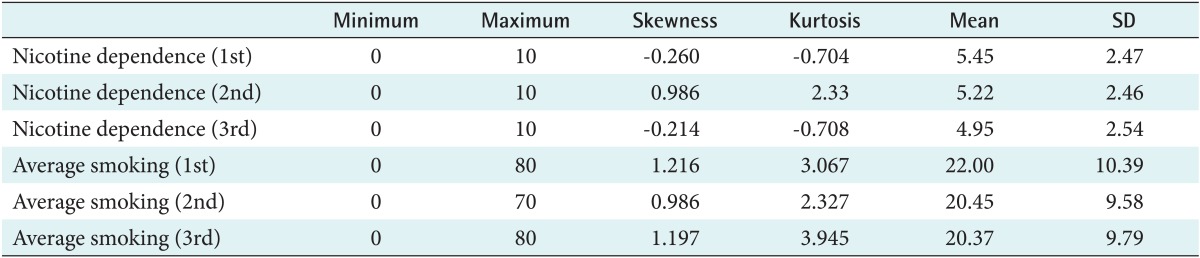
Descriptive statistics of nicotine dependence and average smoking (n = 860)
Prior to analyzing the ARCL model, correlations between nicotine dependence and average smoking were analyzed. Table 3 presents strongly positive (+) correlations between variables.
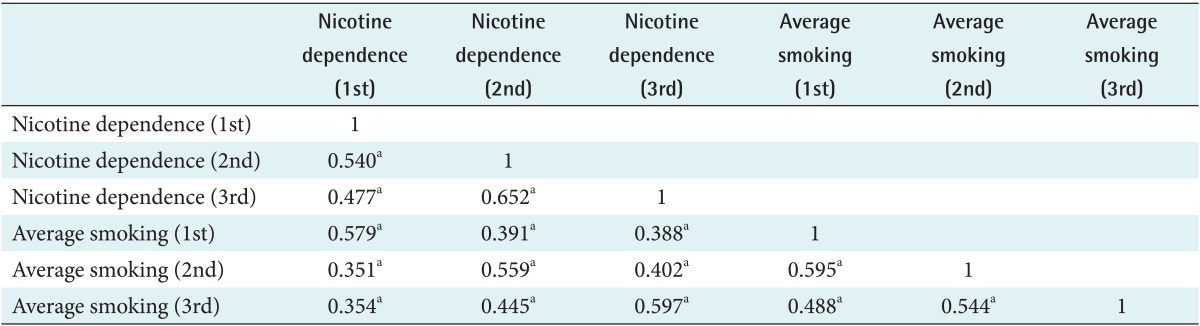
Correlation between nicotine dependence and average smoking
2. ARCL Modeling between Nicotine Dependence and Average Smoking
To test homogeneity of paths and error covariance, the following six competitive models were developed:
Model 1: No constraint to the base model
Model 2: Homogeneity constraint model to the autoregressive coefficient (A) of nicotine dependence
Model 3: Homogeneity constraint model to the autoregressive coefficient (B) of average smoking
Model 4: Homogeneity constraint model to the cross-regression coefficient (C) of nicotine dependence
Model 5: Homogeneity constraint model to the cross-regression coefficient (D) of average smoking
Model 6: Homogeneity constraint model to the error coefficient (E) of nicotine dependence and average smoking
To ascertain the optimal model of the above six models, statistical analyses were sequentially conducted, and its results were compared. Each model was nested; therefore, χ2 tests were viewed as appropriate for the analyses. However, to increase the reliability of the statistical results, other goodness-of-fit indices such as CFI, GFI, NFI, TLI, RMSEA were applied because χ2 tests has been recognized as problematic when related to sample size sensitivity [21,30]. Thus, as applied herein, if the fit indices were not more adverse when any constraint was applied, it was concluded homogeneity was established.
Although homogeneity constraints were added to the paths A-E, the fit indices were not getting worse (Table 4). The impact of the time of [t-1] on the time of [t] proved to be the same with the impact of the time of [t] on the time of [t+1] on all paths. Model 6 did not show a big difference with Model 5; therefore, considering model simplicity, Model 6 was selected as a final model for this study.

Comparison of the autoregressive cross-lagged models
Table 5 presents path coefficients of the finally selected models: Model 6 and a base model. Path coefficients of Model 6 presented in Table 5 indicate that nicotine dependence and average smoking had strongly positive relations over time. Cross-relations flowing from nicotine dependence to average smoking over time were strongly static and vice versa. The impact of average smoking on nicotine dependence (β = 0.109, 0.101) was higher than the impact of nicotine dependence on average smoking (β = 0.085, 0.089). Therefore, it was concluded that it is possible to verify statistical causality by applying the ARCL model of nicotine dependence and average smoking.
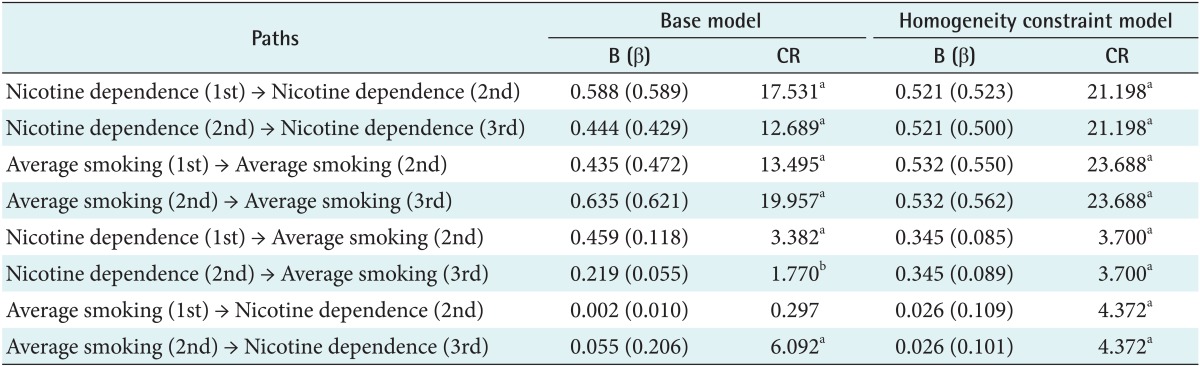
Parameter estimates of the base model and the ARCL Model 6
3. Trajectory Changes of Nicotine Dependence and Average Smoking
A latent growth curve model was developed to explore trajectory changes of nicotine dependence and average smoking. It was noted that both nicotine dependence and average smoking were proved to be linear transformation models (Figures 2, 3).

Linear model of nicotine dependence.
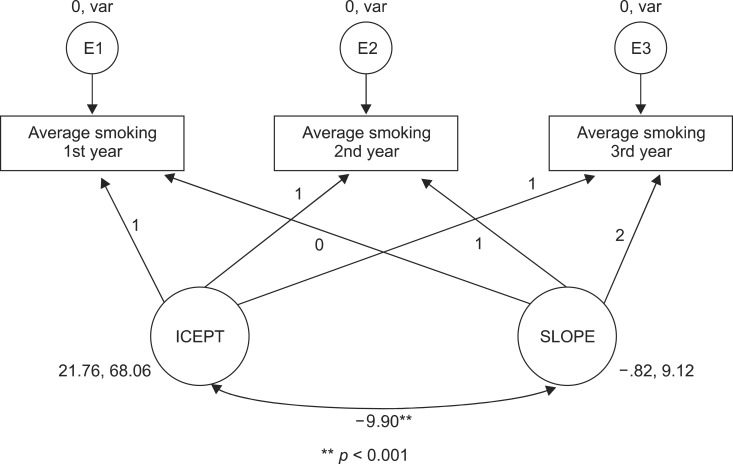
Linear model of average smoking.
In Table 6, the goodness-of-fit of nicotine dependence remained suitable for all other indices except the value of χ2. In case of average smoking, all except the values of χ2 and RMSEA were suitable.

Results from the ARCL model of nicotine dependence and average smoking
Trajectory changes of nicotine dependence showed a linear model which had decreased for the three-year period. The mean intercept of nicotine dependence was 5.454, and it showed a steady decline of 0.247 on average over the period (Table 6). The values of the intercept and the variance of slope were statistically significant. The mean intercept of nicotine dependence had a significant difference between individuals. The slope also had a significant difference between individuals. In addition, the coefficient of correlation between the intercept and the slope was -0.288 indicating that the higher the intercept of nicotine dependence, the lower rate of decline.
Trajectory changes of average smoking also showed a linear model which had decreased for the three-year period. The mean intercept of average smoking was 21.758, and it showed a steady decline of 0.817 on average over the period. The values of the intercept and the variance of slope were statistically significant. The mean intercept of average smoking had a significant difference between individuals. The slope also had a significant difference between individuals. In addition, the coefficient of correlation between the intercept and the slope was -0.398 indicating that the higher the intercept of average smoking, the lower rate of smoking decline.
4. Predictors of Changes in Nicotine Dependence
Figure 4 was proposed as a conditional model in this study. The model was developed based on the results of previous studies [4,13] and the correlation analysis between nicotine dependence and average smoking. In the study, it was specifically analyzed whether attempts for smoking cessation was successful or not and the impact of average smoking on behavior change that lower the level of nicotine dependence over time. A result from the analysis of the conditional model reported that all other fit indices except the value of χ2 (55.410, df = 3) showed suitable fit (NFI = 0.952, CFI = 0.957, TLI = 0.909, RMSEA = 0.090) in the model.

Changes of nicotine dependence over the time period.
Table 7 presented regression coefficients which affect the impact of whether attempts for smoking cessation was successful or not and average smoking on the intercept and the slope. The first success in smoking cessation had a negative (-) effect on the intercept of nicotine dependence (β = -0.085, p < 0.05). It showed a negative (-) effect on the slope (β = -0.183, p < 0.01) as well. In case of the person who was successful in smoking cessation (1st), the intercept of nicotine dependence was low, and nicotine dependence was decreased over time. Success in smoking cessation (2nd) had a negative (-) effect on the slope of nicotine dependence (β = -0.194, p < 0.05). The person who was successful in smoking cessation (2nd) also showed that nicotine dependence was decreased over time. The average smoking (1st) had a positive (+) effect on the intercept of nicotine dependence (β = -0.684, p < 0.01) and a negative (-) effect on the slope (β = -0.425, p < 0.01). Even though a person who had large amount of average smoking showed high nicotine dependence at the initial point measured, and nicotine dependence was decreased over time.

Intercept of nicotine dependence and path coefficients of slope
IV. Discussion
This study was designed to examine the causal relations between nicotine dependence and average smoking for the three year period applying the ARCL to longitudinal data. Results from this study are as follows:
First, nicotine dependence measured at each point was stable over time. Nicotine dependence at the previous point significantly influenced nicotine dependence at future time points. Stated in other terms, nicotine dependence of smokers was an ongoing phenomenon, not a temporary one. Second, average smoking was stable over time. Therefore, average smoking was similar to nicotine dependence. Third, the impact of nicotine dependence on average smoking was significant. Data suggest that average smoking and nicotine dependence had strongly positive relations over time. In addition, the impact of nicotine dependence on average smoking had not changed over time. Lastly, the impact of average smoking on nicotine dependence was significant. Results obtained from this panel data analysis indicate that as average smoking increases, nicotine dependence also increases. These findings remained stable for the three-year period. The impact of average smoking on nicotine dependence was greater than the impact of nicotine dependence on average smoking; therefore, average smoking was the main cause to increase nicotine dependence.
Limitations of this study were as follows:
First, this study used a total score, not an individual item, of the FTND to measure nicotine dependence. Therefore, it was not possible to analyze reliability of the FTND each year. Instead, reliability of a total score of the FTND each year was presented in this study. Second, the models proposed and tested in this study showed the goodness-of fit indices, however, this result does not mean that the study models include the most influential variables on smoking cessation. Therefore, future research is necessary to further establish the relationship between nicotine dependence and average smoking. Additional studies including more influential variables theoretically valid and empirically tested in previous research will lead to the development of new approaches to success in smoking cessation.
In summary, these results support the existing data obtained from previous research that explored the relationships between nicotine dependence and average smoking [3,5,6,11,12,18]. Taken together, they suggest that the impact of average smoking on nicotine dependence is greater than the impact of nicotine dependence on average smoking. Collectively, results suggest that reducing the amount of average smoking in order to decrease nicotine dependence is important to evidence-based policy making. Implications for future research include the need to replicate the study in diverse populations on a global level.
Acknowledgments
This manuscript was prepared by the support of the National Research Foundation of Korea funded by the Ministry of Education, Science and Technology (NRF-2011-413-G0006). The authors acknowledge the contribution from the Ministry of Health and Welfare (MOHW) of Korea, which operated the national smoking cessation program at the community health centers in the nation. The content of this manuscript does not represent the official views of the MOHW.
Notes
No potential conflict of interest relevant to this article was reported.