Factors Affecting Electronic Medical Record System Adoption in Small Korean Hospitals
Article information
Abstract
Objectives
The objective of this paper is to investigate the factors affecting adoption of an Electronic Medical Record (EMR) system in small Korean hospitals.
Methods
This study used survey data on adoption of EMR systems; data included that from various hospital organizational structures. The survey was conducted from April 10 to August 3, 2009. The response rate was 33.5% and the total number of small general hospitals was 144. Data were analyzed using the generalized estimating equation method to adjust for environmental clustering effects.
Results
The adoption rate of EMR systems was 40.2% for all responding small hospitals. The study results indicate that IT infrastructure (OR, 1.48; 95% CI, 1.23 to 1.80) and organic hospital structure (OR, 1.86; 95% CI, 1.07 to 3.23) rather than mechanistic hospital structure or the number of hospitals within a county (OR, 1.08; 95% CI, 1.01 to 1.17) were critical factors for EMR adoption after controlling for various hospital covariates.
Conclusions
This study found that several managerial features of hospitals and one environmental factor were related to the adoption of EMR systems in small Korean hospitals. Considering that health information technology produces many positive health outcomes and that an 'adoption gap' regarding information technology exists in small clinical settings, healthcare policy makers should understand which organizational and environmental factors affect adoption of EMR systems and take action to financially support small hospitals during this transition.
I. Introduction
Healthcare organizations have adopted a variety of information technologies (IT) in South Korea [1,2,3,4]. Among those technologies, the Electronic Medical Record (EMR) system is a core technology that combines various complex information technologies, such as a computerized physician order entry (CPOE) system and a picture archiving and communication system (PACS). This system affects a wide selection of clinical settings in healthcare organizations [4]. An EMR system is defined as "an electronic record of health-related information on an individual that can be created, gathered, managed and consulted by authorized clinicians and staff within one healthcare organization" [5].
EMR systems have various benefits and advantages in healthcare practice [6,7,8,9,10,11]. They save costs by extracting a large number of clinical documents in a timely manner and sometimes prevent human error through techniques, such as alerts, and by providing additional information. As a result, there is great potential for improvement of hospital practices. Although there are many merits to these clinical and managerial systems, their adoption rate has not been very high. The adoption rate has reached 44.9% in Korea [12]. In the United States, the adoption rate of EMR systems in hospitals was approximately 12% in 2009 [13].
The question of why some hospitals adopt EMR systems and others do not is an important one. Adoption is defined as the acquisition or implementation of an EMR system [14]. We need to understand the mechanism of EMR system adoption in order to accelerate system adoption by healthcare organizations. Using an understanding of the adoption mechanism, healthcare politicians can contribute to appropriate political actions that will promote EMR adoption by the healthcare industry.
There have been several studies examining factors that are obstacles to adopting various information technologies, including EMR and CPOE systems. However, there have been no studies targeting small hospitals and the factors affecting EMR system adoption in Korea. There have been several studies on EMR adoption in general and in tertiary hospitals, as well as in ambulatory care clinics in Korea, but not in small hospitals [2,4,15]. Outside of Korea, several studies have been conducted in small primary care clinics and community health centers in the United States on the adoption and use of EMR or Electronic Health Record (EHR) systems, the barriers to EMR system adoption, and experiences of healthcare providers with the use of EMR systems [16,17,18,19,20,21].
Small hospitals are widely distributed and play roles of gate keepers, referring seriously ill patients to tertiary hospitals in Korea's national healthcare delivery system. Small hospitals have several unique characteristics that are different from those of large general hospitals, such as weak financial stability. They usually do not have the financial resources to invest large sums in information technology like expensive EMR systems [19,22]. In addition, they tend to have homogenous group features like small bed numbers and poor organizational structures. An understanding of the current status of small hospitals is needed regarding EMR adoption in order to increase hospitals' rate of EMR system adoption and use in practice settings.
This study aims to examine factors affecting EMR adoption. Compared to large hospitals, small hospitals have been the subject of few studies on the factors affecting EMR adoption. In Korea, small hospitals are defined as hospitals with more than 30 and fewer than 100 beds, according to Korean Medical Law [4]. The objective of this paper is to investigate the factors affecting adoption of EMR systems in small Korean hospitals. Knowledge from this type of study will enable healthcare politicians to determine appropriate political actions for IT advancement in the healthcare industry.
II. Methods
1. Study Subjects
The present study used data from a survey conducted from April 10 to August 3, 2009. After sending a one-time mailing containing an access code and a cover letter explaining the survey purpose and Web address, data were collected from an online website. Some hospitals' IT departments were also directly contacted by phone to solicit their participation in order to increase the response rate. In addition, this study received help in the form of a website advertisement from the Korea Information Technology of Hospital Association (KITHA), which is a professional association composed of chief information officers and IT managers.
Respondents to this study were chief information officers, but anyone who was in charge of a hospital computer system was able to respond if the hospital did not have an IT department. In hospitals that did not have an IT department, most respondents were nurses. There were 1,063 hospitals at the time of the survey and a total of 356 hospitals participated in the survey. The response rate was 33.5%. This study selected small hospitals with more than 30 and fewer than 100 beds. A total of 144 hospitals qualified according to the criteria of this study.
The survey instrument was developed based on a review of the previous literature [23,24,25,26,27,28]. The main dependent variable was EMR adoption status. In order to confirm whether hospitals had actually adopted an EMR system, the survey asked when they had deployed the EMR system; this was defined as the year of EMR adoption. The study provided a definition of the EMR system and asked whether hospitals had fully or partially adopted an EMR system, or not at all. The study also categorized hospitals that reported full or partial adoption of the name system as hospitals with EMR systems, in order to simplify the interpretation of the analysis results.
Table 1 presents a brief description of the major study variables. This study defined 'task complexity' as 'the degree of hospital task diversity' and measured it by 'counting the number of specialty services the hospital provides'. Decentralization of decision-making type was defined as "the degree of IT staff participation level in managerial decision-making"; this measured, on a five-point Likert scale, the average participation levels of IT department staff in an organization's hiring, promotion, program, and policy changes. A higher number means that hospitals had a decentralized decision-making process, in which IT department staff actively participates in the decision-making process. This study also defined 'IT infrastructure' as 'the physical and institutional structures related to information technology'; this was measured by counting the number of 8 areas of hospital information systems: outpatient CPOE, inpatient CPOE, pharmacy drug management and dispensing system, patient charging processing, clinical laboratory work, radiology work management, intensive care unit management, and administrative procedures systems.

Description of major independent variables
Organic versus mechanistic features of hospitals were scaled following a measurement tool from Burns and Stalker [23]. They were measured using a five-point Likert scale, with a higher number indicating that hospitals had organic managerial structures. According to Burns and Stalker's conceptualization, organic organizations have characteristics, such as flexible rules, decentralization of decision-making, and frequent mutual reliance among employees, while mechanistic organizations have the opposite sides of these characteristics [29].
Two different variables to measure market competition were used: the Herfindahl-Hirschman index (HHI) [30] and the existence of true competitors. The HHI was calculated using two variables: the total number of beds in a given area and the actual bed size of the hospitals. With respect to the existence of true competitors, true competitor status was determined based on the difference of the number of beds between any two hospitals within the same local area. This study designated both hospitals as true competitors if the difference in the number of beds between any two hospitals was fewer than 50.
2. Data Analysis
The data was analyzed using the generalized estimating equation (GEE) method with logic function and binomial distribution. Also, we adopted an exchangeable variance-covariance structure to adjust for environmental clustering effects [31,32]. Specifically, this can be modeled using a logistic regression approach with logic function and binomial distribution. The dependent variable was EMR adoption; independent variables were the covariates mentioned above. The GEE model was applied because several environmental factors within the same area equally affected hospital covariates. This study used SAS ver. 9.1 (SAS Institute Inc., Cary, NC, USA) for data analysis.
III. Results
1. General Characteristics of Study Hospitals
Table 2 shows the basic characteristics of the study hospitals according to EMR adoption status. The overall adoption rate of EMR systems was 40.3% for all responding small hospitals. There was no difference in EMR system adoption between small public and private hospitals. Hospital status as a multihospital system (yes vs. no) and having contracts with other hospitals (e.g., group purchasing contracts) were not related to EMR adoption. However, hospitals located in urban areas had significantly higher EMR adoption rates than did hospitals in rural areas.
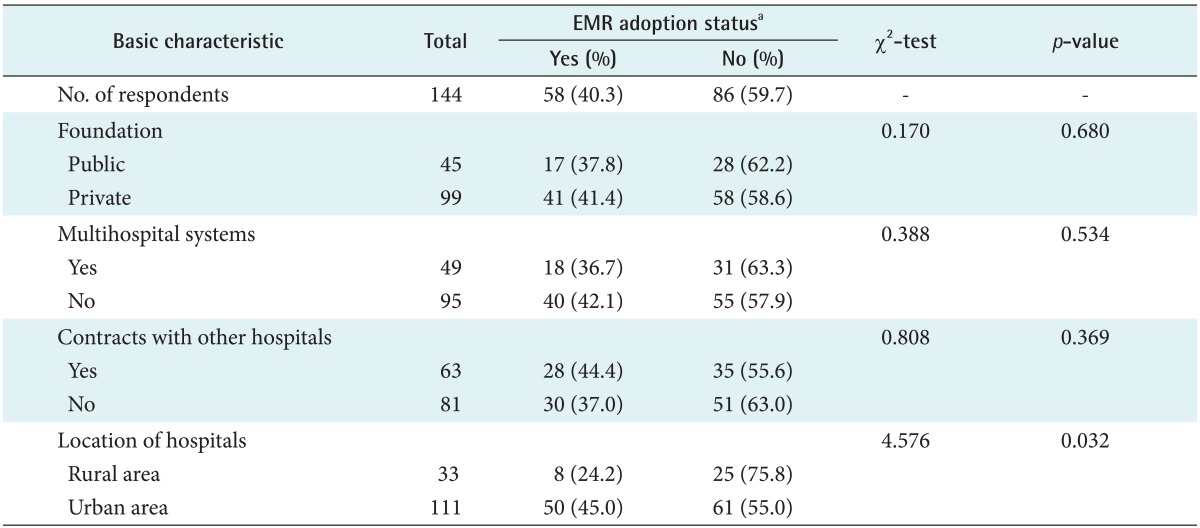
Basic characteristics of study hospitals according to EMR adoption status
2. Internal Features of Hospitals and EMR Adoption
Table 3 shows the relationship between a hospital's internal features and its EMR adoption status. There was no difference in bed size between the two groups. Hospitals adopting EMR systems had higher task complexity than that of hospitals not adopting EMR systems, as measured by the number of medical specialties, but this was not statistically significant. Hospitals adopting EMR systems had significantly higher IT infrastructure (p < 0.001) and organic structural characteristics than did hospitals not adopting EMR systems (p < 0.05).

Internal features of study hospitals according to EMR adoption status
Hospitals adopting EMR systems had a higher number of hospitals within their local area than did hospitals not adopting EMR systems; this was statistically significant (Table 4). This indicates that high competition within the local area might accelerate EMR system adoption by hospitals.
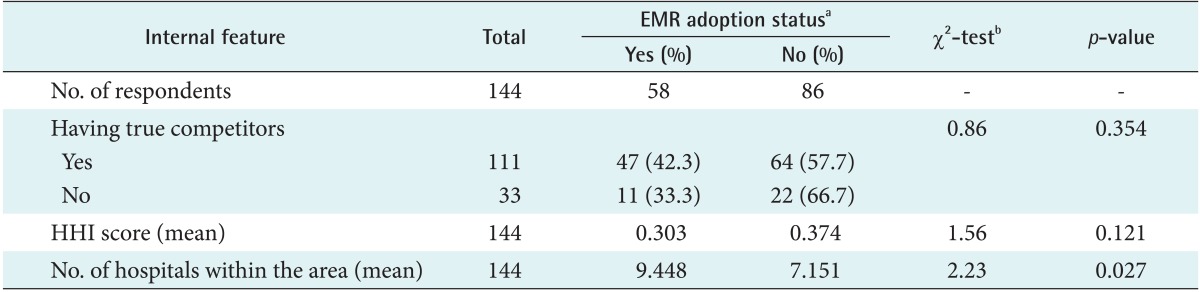
Environmental features according to EMR adoption status
3. Factors Affecting EMR Adoption by Small Korean Hospitals
Small hospitals equipped with high levels of IT infrastructure and with organic managerial structures were more likely to adopt EMR systems than were other types of hospitals (Table 5). EMR adoption was positively associated with the number of hospitals within a given area. A one-unit increase in IT system was associated with 48.5% higher odds of adopting an EMR system, which was statistically significant (95% CI, 1.23 to 1.80; p < 0.005). For a one-unit increase in the score of structural features toward an organic form, the odds of EMR adoption were estimated to increase by a multiplicative factor of 1.857 after controlling for hospital covariates (95% CI, 1.07 to 3.23; p < 0.05). A one-unit increase in the number of hospitals within a given area was associated with 8.2% higher odds of adopting an EMR system (95% CI, 1.01 to 1.17; p < 0.05), which was statistically significant.
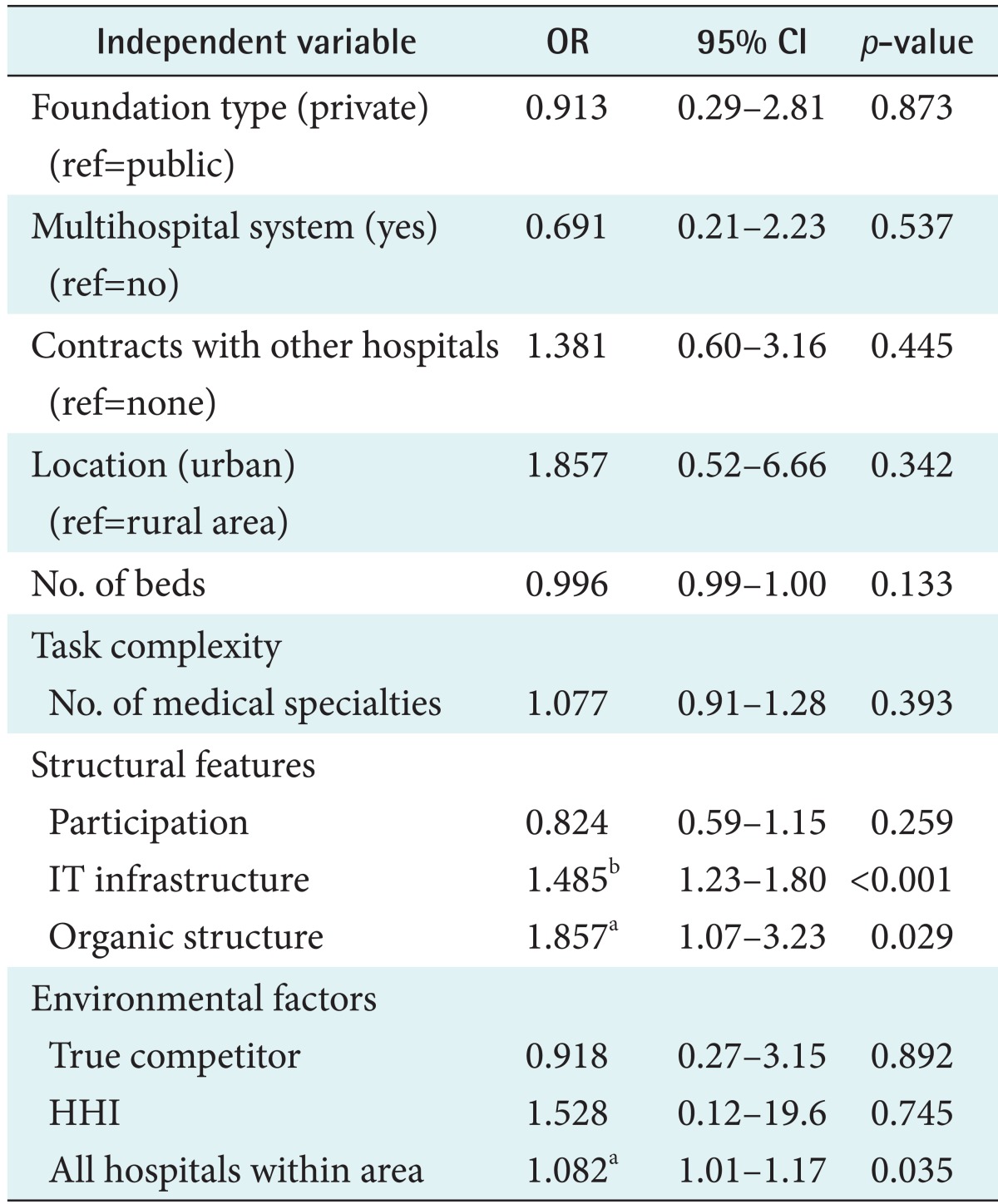
Factors affecting EMR adoption by small Korean hospitals
IV. Discussion
The present study primarily investigated the factors affecting EMR adoption in small Korean hospitals. Although several studies have investigated EMR adoption in Korea, there have been few studies targeting small hospitals and the internal features related to EMR adoption. Policy makers need to determine how to motivate small hospitals to invest financial and human resources in EMR system adoption in order to address the 'adoption gap' in small clinical practice settings with regard to health information technologies [19]. Because small hospitals lack large financial investment resources for their hospital facilities and healthcare IT, the present study results could provide meaningful information to assist governments in supporting small hospitals with regard to EMR adoption.
This study found that the EMR adoption rate of small hospitals was 40.3%, which is slightly higher than that found in previous studies. According to a previous study investigating EMR adoption, the overall adoption rate of general hospitals was 38.0% [2], which was an almost identical adoption rate. That study was conducted in 2004 and the study subject was general hospitals.
Regarding the four factors of general hospital characteristics, only hospital location was significantly related with high adoption rate. Hospitals located in urban areas had higher adoption rates than did hospitals in rural areas. However, when we looked at the relationship between general and internal features of small hospitals and EMR adoption, none of the general characteristics were significant factors in EMR adoption. Location of hospitals might be a confounding variable affecting EMR adoption. Further study is necessary to determine how this variable is related to other internal features of small hospitals.
Among hospital internal features, IT infrastructure and organic structural form were factors critically affecting EMR adoption. These findings were also found in a previous study [12]. Several theoretical arguments support this finding. Hospitals with greater IT infrastructure can more easily invest in EMR systems because they have an environment that is accepting of new and highly complex EMR technologies. Organic organizational structures with characteristics emphasizing horizontal communication are accepting of new ideas from employees, which might create an environment in which EMR systems could be easily installed. Regarding external environmental factors, HHI and the existence of true competitors were not related to EMR adoption. Only the number of hospitals within an area was significantly related to EMR adoption. This finding was also observed after controlling for a hospital's general characteristics. A similar finding was also found in a previous study [12].
The present study has two limitations. First, this study had a small sample size. Given that there are 778 small hospitals in Korea, the number of responding hospitals, 144, represents only 19.0% of the total study population. Second, interpretation of the study results should be confined to small Korean hospitals.
This study suggests several policy implications. First, as mentioned above, cash investment in EMR systems presents a bigger challenge to small hospitals than it does to large hospitals, which generally have larger resources. It may therefore be necessary for governments to provide financial support to small hospitals. Small hospitals are widely distributed in the market and an 'adoption gap' for healthcare IT exists in small practice settings [19]. Second, as can be seen in the present study results, the adoption rate of small hospitals is relatively low compared to that of larger hospitals [2], such as teaching hospitals. In the market, EMR adoption rates might increase with government financial support. This is particularly important for healthcare information exchanges (HIE) with regard to the sharing of results of lab or imaging tests. Practical impacts of HIE could be achieved if large and small hospitals had their own EMR systems. Governments should create political initiatives to support the adoption of EMR systems by small hospitals. Third, this study only included several hospital structural factors. Thus, additional studies including more varied structural covariates are necessary. In addition, further studies are needed to investigate how small hospitals' EMR adoption factors differ from those of large hospitals.
In conclusion, IT infrastructure, organic managerial structure, and environmental complexity were critical factors affecting EMR adoption. This study empirically verified that decision making structure and number of hospitals, rather than market competition based on bed size in a given area, were important EMR adoption factors.
Acknowledgments
The authors express their deep thanks to Dr. Stuart M. Speedie, a member of the faculty at the Health Informatics Graduate Program of the University of Minnesota, for his comments, advice, and support.
Notes
No potential conflict of interest relevant to this article was reported.