Current National Approach to Healthcare ICT Standardization: Focus on Progress in New Zealand
Article information
Abstract
Objectives
Many countries try to efficiently deliver high quality healthcare services at lower and manageable costs where healthcare information and communication technologies (ICT) standardisation may play an important role. New Zealand provides a good model of healthcare ICT standardisation. The purpose of this study was to review the current healthcare ICT standardisation and progress in New Zealand.
Methods
This study reviewed the reports regarding the healthcare ICT standardisation in New Zealand. We also investigated relevant websites related with the healthcare ICT standards, most of which were run by the government. Then, we summarised the governance structure, standardisation processes, and their output regarding the current healthcare ICT standards status of New Zealand.
Results
New Zealand government bodies have established a set of healthcare ICT standards and clear guidelines and procedures for healthcare ICT standardisation. Government has actively participated in various enactments of healthcare ICT standards from the inception of ideas to their eventual retirement. Great achievements in eHealth have already been realized, and various standards are currently utilised at all levels of healthcare regionally and nationally. Standard clinical terminologies, such as International Classification of Diseases (ICD) and Systematized Nomenclature of Medicine - Clinical Terms (SNOMED-CT) have been adopted and Health Level Seven (HL7) standards are actively used in health information exchanges.
Conclusions
The government to New Zealand has well organised ICT institutions, guidelines, and regulations, as well as various programs, such as e-Medications and integrated care services. Local district health boards directly running hospitals have effectively adopted various new ICT standards. They might already be benefiting from improved efficiency resulting from healthcare ICT standardisation.
I. Introduction
Many nations have invested in the standardisation of healthcare information technologies (HIT). Healthcare information exchanges (HIE) or sharing of clinical data is simply not feasible without appropriate standardisation. Without having the HIE, we cannot expect to establish and operate a cost effective and sustainable healthcare system that has high quality of care [1234]. Therefore, many countries have put significant effort in HIT standardisation and are adhering to certain standardisation processes [567].
Although each nation has those interests in HIT standardisation, the structure and process of the standardisation are a little bit different. In the United States, the private sector play an important role in HIT standardisation. There are many standard developing organizations (SDOs), such as the American Society for Testing and Materials (ASTM), the American Society of Mechanical Engineers (ASME), Health Level Seven (HL7), and so on [8]. Each organization has its own standardisation process and structure. For example, ASTM accepts ideas and reviews and creates standards, which then become the national standards [9]. Regarding HIE, the Continuity of Care Record (CCR) is a key standard from ASTM for the purpose of defining a standard summary record at a point in time to facilitate clinical communication between providers. HL7 developed the Clinical Document Architecture (CDA), which defines a standard structured definition of a signed clinical document to facilitate document-based HIE between Electronic Medical Record (EMR)/Electronic Health Record (EHR) systems. In 2007, the Continuity of Care Document was created with convergence of CDA and CCR by the two SDOs [10]. The American National Standard Institute (ANSI) is a non-profit organization founded in 1981. It credits various SDOs and approves standards of the private sector's efforts and outputs [11]. The Office of National Coordinator for Health Information Technology under the Department of Health and Human Services was founded in 2001 to support the private sector and to facilitate the adoption of developed standards in the healthcare industry [1213]. Thus, the private HIT sector is taking a dominant role in the area of standards development and adoption in the United States, and the government is actively supporting this.
The national standards body of the United Kingdom is the British Standards Institute (BSI) founded in 1901. It is a nongovernmental not-profit organization. BSI has established the vast majority of standards at the national level, including HIT [1415]. In Australia, Standards Australia (SA) is in charge of developing and approving all kinds of standards including HIT. It is also a non-governmental SDO. SA has several internal parts, such as the Accreditation Board for Standards Development Organizations, Standards Australia Council, and the Standards Development Committee [161718].
In contrast, the government of New Zealand is directly involved in standards development in HIT and runs the Health Information Standards Organisation (HISO). It may be more effective because several empirical studies have shown that government power usually has a strong influence on the healthcare industry [192021]. The government of New Zealand has already established governmental organizations regarding HIT and has created various HIT standards, which it updates regularly. Those guidelines on HIT standardisation have been actively adopted by independent hospital management authorities [222324].
The objective of this study was to review the HIT standardisation and progress of New Zealand. Specifically, this paper describes how governmental organizations for healthcare ICT are organised, how they work, and how they transfer current HIT standardisation to the healthcare industry. This kind of governmental involvement has various political implications on how healthcare politicians document policies of HIT and presents as an opportunity to provide a benchmark for other nations. Thus, this study could provide many other countries with meaningful implications regarding HIT standardisation.
II. Methods
We reviewed reports regarding the HIT standards and standardisation processes published by New Zealand government agencies, including the Ministry of Health, Health IT Board, and HISO. In addition, we visited their websites and reviewed materials related to HIT standards. Then, we summarised these materials focusing on governance structures, standardisation processes, and their outcomes. Finally, we investigated several important issues regarding the current HIT standardisation status of New Zealand.
III. Results
1. Governance of HIT Standards in New Zealand
The governmental department supporting the national healthcare service system in New Zealand is the Ministry of Health operating through the National Health Board (NHB) (Figure 1). The former has direct responsibility for delivering public healthcare to the people and supports the latter. The NHB is an advisory board for the former and is responsible for overseeing various activities of District Health Boards (DHBs) including funding, monitoring, and planning [25]. The National Health IT Board (NHITB) under the NHB is the governing body for health information standards in New Zealand. It has a sub-committee called the HISO which provides important advice to the NHITB regarding the development and adoption of national HIT standards [26].

HISO has a group of seven committee members, including a chairperson. HISO collaborates with the Health Sector Architects Group, comprising about 30 experts from various sectors of the healthcare setting. The HISO's responsibilities include providing advice to the NHITB about the development of health information standards, identifying and adopting relevant international standards, managing and ensuring standard development process with an open and consistent way, and ratifying new standards and withdrawing old ones [26].
There are 20 DHBs that closely collaborate with the NHITB. They have some obligations to comply with HISO standards under the parliamentary funding agreement called the Operational Policy Framework (OPF). The OPF 2014/15 Section 11.2.3.c requires:
"…DHBs to … Proactively support the development and adoption of Health Information Standards Organization (HISO) standards by: adhering to and meeting the requirements of all published HISO standards, identifying and reporting on needs or opportunities for new standards and updates to existing standards, participating in the development or enhancement of standards, supporting trial implementation of interim HISO standards (p.103)." [23].
2. Use of EMR/EHR Systems in Hospitals and Primary Care Settings
New Zealand is divided into four health regions, each with a number of public hospitals and primary health organizations. Under the National Health IT Plan, regions are responsible for delivering a regional hospital patient administration system, regional hospital/community clinical workstation/portal and regional clinical data repository. Hospitals operate the usual clinical specialty and clinical support systems, including Radiology Information System/Picture Archiving and Communication System (PACS), Laboratory Information System, and pharmacy management. Hospitals are implementing the same software for medicines reconciliation, medication management and e-discharge. Hospitals tend to operate best-of-breed solutions rather than integrated product suites. However, the sector places a lot of importance on systems interoperability, and that is where much of governmental standardisation effort is directed.
All general practitioners (GP) use an EMR system, called practice management systems, and many now offer a patient portal. Access by hospital emergency departments and other providers to GP-held patient data is enabled by provider portals, which are also now in rollout around the country. In addition to regional and primary care solutions, there are national solutions, including the National Health Index (patients) and Health Provider Index. New Zealand has implemented a national clinical assessment application based on the Comprehensive Clinical Assessment for Aged Care (interRAI) methodology, and the government is rolling out a centrally hosted maternity clinical information system.
3. Current Standards on HIE in New Zealand
HL7 version 2.x message-based HIE has been operational for many years in the area of lab results, discharge summaries, primary care medical records and e-referrals. While this has been very successful, New Zealand is now moving towards web service-based HIE for new applications. The Interoperability Reference Architecture [28] was authored by an expert group in 2011, and the essential parts were standardised as Health Information Exchange Architecture Building Blocks and ratified as an interim standard by the HISO [29]. This comprises three pillars:
1) HISO 10040.1 is about clinical data repositories and their interfaces. It states requirements for a particular set of document-sharing services based on the IHE XDS integration profile. XDS defines methods to store, locate and retrieve information from multiple sources or repositories (as in regional and national levels). The central mechanism used to achieve this is a registry providing a consolidated index over all content within the ecosystem.
2) HISO 10040.2 is about establishing a single content model for supporting the semantics of information exchange. It is based on CCR specification and prescribes a set of detailed clinical models expressed as openEHR archetypes [30].
3) Finally, HISO 10040.3 is about the use of HL7 CDA structured documents as the common currency of exchange-the payload.
This new service-oriented HIE approach is underpinned by a virtual private network called Connected Health, which is provided by a number of telecommunication providers. The new model of information sharing is to use regional clinical data repositories to make shared clinical documents available to distributed care teams, using a record locator service to index the collective content of all repositories and make content findable by clinical workstation and patient portal systems. New Zealand is also implementing a national e-prescription broker system for prescribing and dispensing medications in the community. This system links GPs and community pharmacies, and it will also be used to convey hospital discharge prescriptions. Government has developed a Systematized Nomenclature of Medicine - Clinical Terms (SNOMED CT)-based national medicines terminology and a national medicines formulary to enabler e-prescribing in the hospital and community.
Regarding HIT standardisation, full standardisation of systems, hardware and software across the entire health sector is not the ultimate goal of the NHITB. The NHITB focuses on the standardisation of health information representation, security and exchange. The SNOMED-CT has been accepted by HISO and has an endorsed standard status.
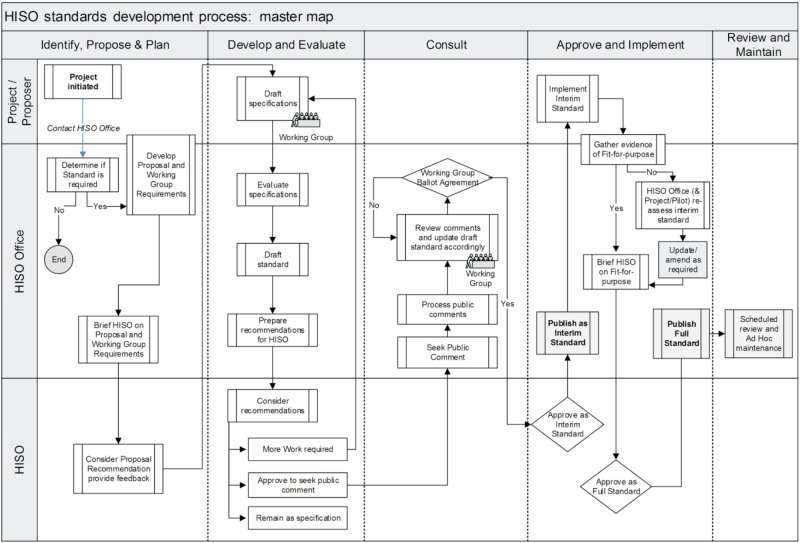
4. Process of the HIT Standardisation
The HISO plays a critical role in creating HIT standards from their inception to their adoption. Figures 2 and 3 provide an overview of the development, review and maintenance of HISO standards [24]. During this time, HISO is supported by DHBs. They are actively involved in the HISO Standards development process.

5. Programs of HISO for National Health ICT Standardisation
The HISO (through the National Health IT Board) is running a Standards Adoption and Compliance Program. This is in its first year of operation. Current efforts are researching and establishing a detailed knowledge of the present situation in the health provider community. Analysis of a sample survey is underway with results being reported back to DHBs. Future steps are still in development.
Figure 4 shows the work programmes in order of priority. Critical priorities are those agreed by sector leaders and the National Health IT Board, which take precedence over all other new IT priorities. These critical priorities include the New Zealand electronic Prescription Service (NZePS), electronic Medicines Reconciliation (eMR), Clinical Workstation (CWS), and Clinical Data Repository (CDR). Important priorities are determined based on the existence of strong local or regional needs or requirements, and these include the electronic Prescribing and Administration (ePA) of medicines and the New Zealand Universal List of Medicines (NZULM), eReferrals and eDischarges. Emerging priorities are the areas of emerging work so health organisations can make an early start on them such as eEnrolment, telehealth, and so on.

6. Nationally Standardised EMR or EHR Systems
Regions have autonomy to implement patient administration, clinical data repository, clinical specialty and clinical support systems of their own choosing. Regional systems are required to integrate with the National Health Index and Health Provider Index systems. There are nationally endorsed choices in certain classes of software, including clinical workstation and medications management. The pervasiveness of this software and the desirability of a common user interface for the highly mobile clinical workforce were behind these choices.
IV. Conclusion
This study reviewed the governance structure, standardisation processes, and current standards of HIT in New Zealand. Through this study, we could verify that the government of New Zealand plays an important role in HIT standardisation. Modern healthcare organizations heavily depend on HIT standards and rules [31].
Important findings from this study could be summarised as follows. First, the government of New Zealand, unlike those of other countries, has had specific HIT bodies to drive and support standardisation, including the National Health IT Board, the HISO and the Health Sector Architects Group, which actively participate in the standardisation processes. They collect good ideas from the healthcare industry and the public sector and then develop various HIT standards. Second, there are clear internal guidelines and procedures for standardisation. Third, we also could see that there were various specific outcomes of healthcare HIT, such as e-referral systems, e-prescribing systems, and so on. Those programs are planned, developed, and implemented by direct government involvement.
New Zealand's governmental structures and processes may be a direct and efficient way of achieving the benefits of HIT standardisation because government power has a strong influence on markets, and many healthcare organizations are under government control, such as public and tertiary hospitals. Several empirical and theoretical studies have shown that government power and influence is the strongest driving force [192021].
This study suggests several meaningful future implications. Firstly, we wish to investigate whether there would be any beneficial effect of HIT standards on healthcare outcomes, such as minimising errors in healthcare organization. We are also interested to see how other countries could benchmark with the achievements of HIT standardisation as in New Zealand. Conferences or international cooperation for sharing experiences and information with lagging countries could lead to valuable outcomes.
Finally, we believe this kind of active government involvement could bring about many benefits in terms of reducing errors and improving the quality of care at the national level. We expect that this study will provide a benchmark for those lagging countries regarding ICT standards and standardisation processes.
Acknowledgments
We would like to acknowledge Alastair Kenworthy (Principal Sector Architect, Ministry of Health) and Ted Christiansen (Principal Advisor, Ministry of Health) for their substantial contributions and for critically reviewing the manuscript. We thank Emmanuel Jo, Principal Technical Specialist of Health Workforce New Zealand, for help in getting important information on HIT and his insightful comments on the manuscript. This work was supported by the Health Insurance Review & Assessment Service (HIRA)'s Research Fund (13-02-01-06).
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.