I. Introduction
Well-dying, a term referring to dying with dignity, has become prominent as the world is rapidly becoming an aging society [1]. In the same line, a growing number of terminally ill patients prefer hospice care to maintain their quality of life instead of going through long-suffering treatment to prolong their life by a few months or years [2]. Therefore, hospice referral for terminally ill cancer patients is becoming popular and crucial [3].
According to a World Health Organization report, in developed countries, 60% of the deaths by cancer require hospice care, and 40% of the deaths are targeted for it. Among them, 34% were cancer patients [4]. In Korea, 7 out of 10 people responded they would use hospice if they were in a terminal condition, and almost 100% of doctors agreed with it. In addition, according to the satisfaction survey of hospice care, 85% answered that the services were satisfactory [5]. Patients with a life expectancy of 6 months or less can request hospice care if they state and sign that they no longer want to continue chemotherapeutic treatments [6].
The health information exchange (HIE) system developed by the Ministry of Health and Welfare (MOHW) [7] facilitates hospice referrals. In the case of terminally ill cancer patients, efficient and accurate data exchange is particularly important because of the consquences of wrong cancer treatments [8].
Our study focused on examining the current hospice referral system for terminally ill cancer patients and analyzed the problems and requirements of the medical staffs so that we could suggest a more practical and efficient referral system for terminally ill cancer patients requiring hospice care. Therefore, we prepared a data form to collect information about hospices. Additional data essential for hospice referral for terminally ill cancer patients are newly defined based on the existing HIE data form. Additionally, we proposed implementing the Consolidated Clinical Document Architecture guidelines developed by Health Level 7 (HL7 CCDA). It is an international standard for interoperability that provides a framework for the exchange, integration, sharing, and retrieval of electronic health information. Based on these changes, a new hospice referral system for terminally ill cancer patients was proposed.
II. Methods
1. Hospice Status and User Requirements
We conducted a survey to the staffs of hospices that asked for a detailed hospice status such as the retained medical instruments and patient admission policies. So far, there has been no studies on hospice status and patient admission policies although each hospice has a different patient admission policy. This often causes delays in hospice referral due to inappropriate matching between the hospice and the patient.
The questionnaire consisted of 7 categories: Hospice type, Volume of wards, Hospital information system, Patient admission policy, Medical service coverage, Patient admission process, and Treatment information. We sent the survey through FAX and collected the responses from the respective hospices by phone, e-mail, or FAX.
Interviews were conducted of physicians, nurses, and HIE experts in tertiary hospitals to examine the current hospice referral flow for terminally ill cancer patients; the interviewees were asked about their hospice referral experiences and the additional requirements they needed to improve the existing system.
To analyze the results of the surveys and interviews, we established a task-force team (TFT) comprising 7 experts from various fields to reflect different viewpoints: 3 physicians, 2 hospice nurses, 2 tertiary hospital nurses, and 3 information and communications technology (ICT) experts. The TFT held regular meetings every 2 weeks for 4 months. They analyzed the survey and interview results, diagnosed the problems within the current hospice referral system for terminally ill cancer patients, and developed strategies to improve the existing process.
2. Design of the Hospice Referral System for Terminally Ill Cancer Patients
After identifying the problems and requirements, a hospice referral scenario for terminally ill cancer patients was designed. To reflect the needs of the users and to consider the situational context, we focused on attempting to minimize the physical and psychological burden of all participants. Through regular task force meetings, we elicited feedback from the TFT as an iterative process to drive a new scenario aligned with the needs and values of this project.
3. Data Standardization
To ensure interoperability of the newly added data set in the HIE form, we searched for an appropriate template to represent each content in a standardized way. Among a variety of international standards for health records, we proposed the HL7 CCDA, a popular and flexible international standard [9], with a wide range of contents. Furthermore, the existing HIE also follows the HL7 standard [10]. Therefore, it would maintain the integrity of the total dataset. Data contents difficult to match with the existing version of the HL7 Clinical Document Architecture (CDA) Release 2 standards are presented in the form of a narrative block of the CDA document. Narrative blocks allow ‘human-readability’ of a CDA document. Within a document section, the narrative block represents contents rendered for viewing [11].
III. Results
1. Hospice Referral System for Terminally Ill Cancer Patients
A total of 6 hospices completed the surveys, and 3 physicians, 2 nurses, and 2 hospital staff from a tertiary hospital were interviewed. Seven categories were defined as essential data for establishing hospice data. Collected questionnaires and interview results were analyzed by the TFT. The results of the investigation are as follows.
1) Status of hospice referral for terminally ill cancer patients in Korea
There had been no medical reimbursement policy to cover hospice services by the National Medical Insurance until 2015 in Korea [12]. However, since July 15, 2015, the Health Insurance Review and Assessment Service (HIRA) of Korea started a new health insurance policy on hospice service for cancer patients to encourage hospice care [13]. According to the report of the Health and Social Welfare Review of Korea, the number of inpatients in hospice care facilities is gradually increasing. Additionally, the hospice utilization rates are increasing among cancer patients [14]. Based on these statistics, health and social welfare researchers have predicted that 27.9% of cancer patients are going to receive hospice care by 2020.
2) Current hospice referral process for terminally ill cancer patients
The current hospice referral process for terminally ill cancer patients through referral centers in tertiary hospitals is as follows: (1) If an inpatient with cancer and a life expectancy of 6 months or less states that he/she no longer wants to continue anti-cancer treatment, (2) the patient is guided to the hospice counseling center of the hospital to request for a referral. The counselor calls hospices to check whether they have an open-bed and informs the guardian. (3) From among the hospices that have open-beds, the guardian and patient select one and inform the counselor about their choice. The counselor then guides them to the Hospital Referral Center. (4) The patient or the guardian requests for referral documents from the Hospital Referral Center. (5) The referral center arranges a reservation and provides the care record summary (CRS), recent exam results, and CDs. Additionally, the patient/guardian signs a consent form for the HIE. (6) Thereafter, the guardian takes all the medical records and visits the hospice to request admission consulting. (7) A nurse or consultant of the hospice transmits the patient records to the medical staff. (8-1) If the patient is admitted, the patient is discharged from the tertiary hospital and proceeds with the admission process in the hospice. (8-2) If not, the guardian returns to the tertiary hospital and restarts the process from (2) until the patient is admitted to a suitable hospice (Figure 1).
There is a HIE system to make the patient exchange between institutions easy and efficient. However, the current standard has a limitation that cannot cover important patient information. Guardians have to visit various offices to get copies of all medical records because they do not know what kind of documents they need. The medical records are voluminous and may confuse the consulting manager at the hospice, which may result in under-recognition of important information regarding the care needed for the patient. In addition, lack of information about hospices makes it difficult to select a suitable hospice for each patient.
2. Process Problems and User Requirements
In all, 10 categories and 40 data items are newly suggested for addition to the existing HIE document form. Based on the current system and the results of the investigation on the process, the TFT identified the following two problems that may result in complications and delays in the referral process.
1) A narrow range of patient information in the current HIE form
The existing HIE form does not provide enough specific information to maintain the continuity of patient care for terminally ill cancer patients. To maintain the continuity of patient care, specific information about the patient's current status and treatment is needed, such as the status of the terminally ill (no option for active anti-cancer treatment; condition of gradual deterioration) and the use of specific drugs (restricted antibiotics, inotropics, and non-reimbursement drugs). Furthermore, knowing a patient's (1) mental status data, whether he or she is mentally alert, (2) functional status data, such as vital sign stability or ventilator usage, ascites/pleural catheter insertion, and (3) data on whether the patient has contracted any infectious disease, and so on, are all crucial in the care for cancer patients. For patient admission consulting and sustainable treatment, each facility requires various medical records. However, because the current HIE form does not cover many of these, the guardian should visit each office to get copies of all the medical records. This takes up the time and resources of the guardian both physically and psychologically.
2) Lack of information about hospices
When the counselor of a palliative care center in a tertiary hospital chooses a facility, he or she calls the hospice to check whether there is an open bed. Even if there is an open bed, there is a possibility that the patient is refused admission because each facility has different patient admission policies and service coverages. When reserving a facility, the counselor will consider these factors to prevent a guardian from having to repeat the admission process multiple times.
Based on the results of the problem analysis, the expert panel identified three outputs to strengthen the current system: they (1) re-defined the HIE form, (2) made an entity definition to collect practical information about hospices and (3) re-designed the hospice referral scenario for terminally ill cancer patients.
3. Design of the Hospice Referral Scenario for Terminally Ill Cancer Patients
This scenario is designed based on the two research outputs mentioned above. The newly designed process is as follows: If an inpatient with cancer and a life expectancy of 6 months or less states that he/she no longer wants to continue anti-cancer treatment, (1) then the hospital referral center staff checks the information on the hospices taking into consideration the status of the patient, admission policies of each hospices, open-bed status, and treatment coverages. After selecting adequate candidates, the staff informs the patient/guardian. The patient/guardian agrees to participate in the HIE and selects one hospice. (2) Through the HIE system, the tertiary hospital staff sends the patient information to the hospice. (3) The staff in the hospice receives and checks the information before deciding whether the patient can be admitted. After making a decision, the hospice informs the tertiary hospital staff and notifies them of the available time to visit. (4) After receiving the reply, the tertiary hospital staff informs the patient/guardian to arrange a visit. (5) After arranging an appointment, the patient/guardian visits the hospice at the appointed time, and the patient is discharged from the tertiary hospital to proceed with the admission process into the hospice (Figure 2).
In this scenario, the staff at the tertiary hospital can search for suitable hospices. The guardian does not have to go back and forth between hospices because all the patient information is delivered to the hospice institution in advance through the HIE system. Additionally, the staff at the hospice can easily access the medical records important for caring for the patient.
4. Data Standardization
We matched and suggested each content with a global standard to ensure the interoperability of the newly added contents in the referral form.
1) HIE form for hospice referral for terminally ill cancer patients
(1) Basic information
The header section of the standard HIE form describes the basic patient information [15]. However, all the interviewees responded that they would contact the guardian instead of the patient. Therefore, guardian information is proposed to be added to the header section, and all optionality of the sub-contents are set as an essential value, which means they ‘must be filled in’. There are three options: O, R, and R2. O refers to data that are completed on the HIE form depending on the decision of the medical staff. R refers to data that are essential and required on the HIE form, and R2 refers to data that are optional on the HIE form.
(2) Medical information
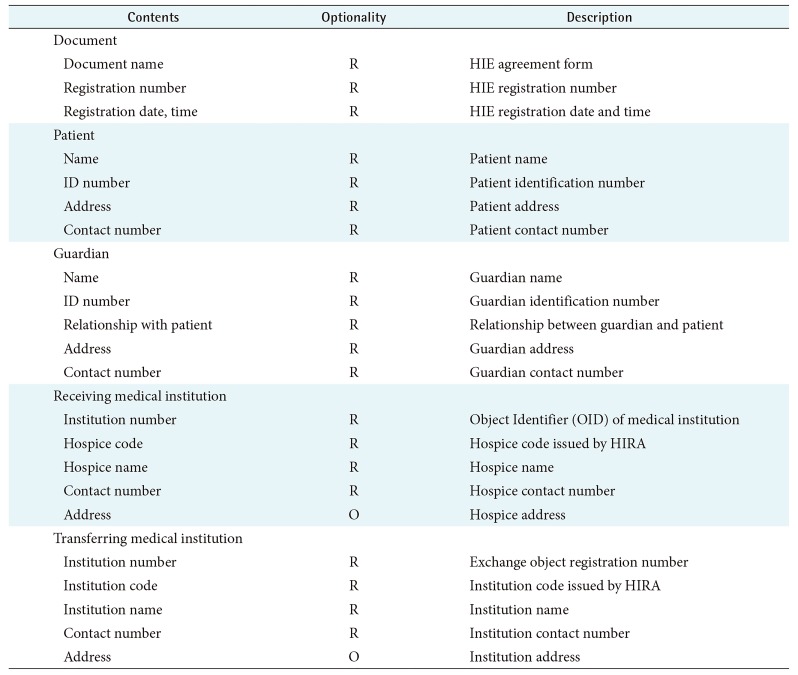
The body section of the current HIE form contains the medical information of the patient such as diagnosis, examinations, investigations carried out, prescription, etc. Except for these, the status of the patient, specific drug information, and the treatment information such as ascites or pleural catheter insertion are also important information to assess the admission and continuous care of a patient. Therefore, we suggest adding these datasets to the current HIE form, and the optionality of all data are set as ‘will be completed if necessary’. Some of the data are needed to make sure whether the facility has the specific treatment instruments that are vital to care for patients, such as ventilators, inotropic support, etc. (Table 1).
(3) Physician's note
Due to the MOHW's legal amendments, a physician's note must be submitted to certify that the patient is terminally ill with a life expectancy of 6 months or less. Therefore, the standard HIE form is supplemented with the physician's note block. Because the physician's note will include a brief narrative of the clinical findings and patient status, it is set in an unstructured form, and documents and images can be attached to it (Table 1).
(4) HIE agreement
When exchanging the health information of patients, the consent of a patient is essential. However, because of the patients' poor general condition, most patients find it difficult to visit the referral center by themselves. Therefore, a guardian who can prove his or her relationship with the patient can sign the consent form instead of the patient. Therefore, we suggested adding the consent section to the current standard HIE form. Once the patient or the guardian agrees to share the medical records of the patient, the Master Patient Index (MPI) number to identify the patient is issued, and the private information of patient is protected (Table 2). The MPI is an index issued to each patient for maintaining confidentiality about each patient registered in the system. In this system, the patient document created is referred to by its MPI number.
(5) Document standard
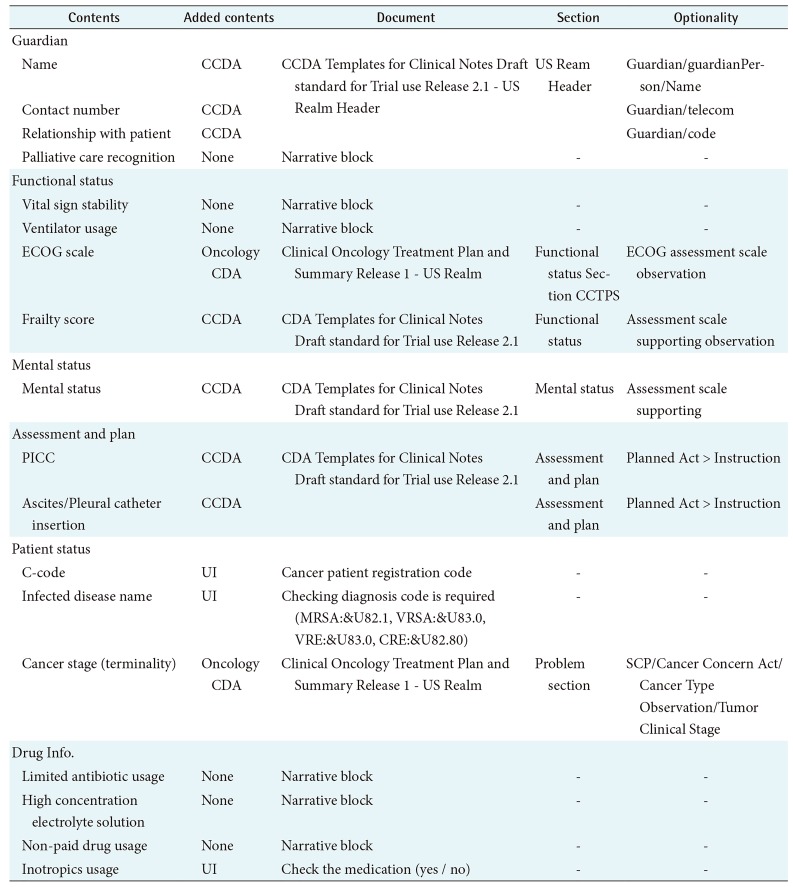
We proposed to adopt the HL7 CCDA international standard because it can cover a wide range of contents, and the existing referral form designed by the MOHW of Korean government also follows the global HL7 standard. In the case of data not defined by the HL7 CCDA, they are set as a part of the narrative block. The narrative block is the area in the CDA document that people can read (Table 3).
2) Entity definition to collect practical information about hospices
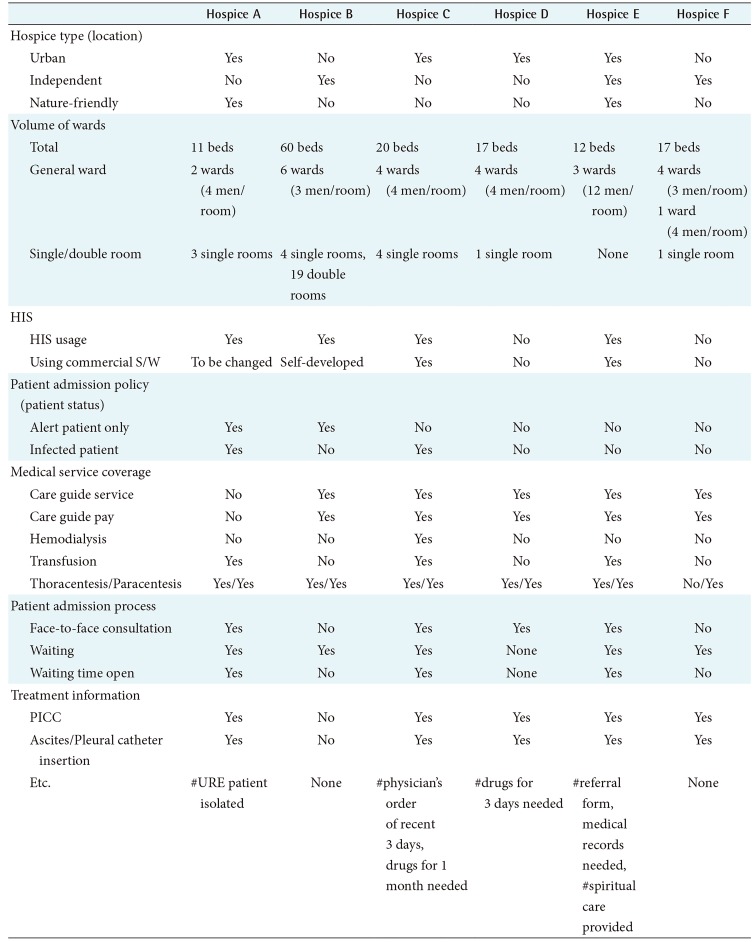
We defined datasets for collecting hospice information needed to select facilities that are suitable for the patients' needs based on the requirements of the institutions. A total of 7 categories and 21 items were defined except for the information on the interviewer and the basic information on the hospice organization.
The suggested data categories and contents are as follows: facility type, volume of wards, the kind of HIS, patient admission policy, range of services provided, patient admission process, and treatment information. After defining the datasets, information corresponding to the data model in 6 hospice institutions was collected (Table 4).
IV. Discussion
About 15% of cancer patients presently receive hospice care, and the rate is gradually growing. However, hospice referral for terminally ill cancer patients is not a smooth process; instead, there are frequent delays. There are considerable challenges in exchanging patient medical records and selecting adequate hospices. The obstacles are in the existing standard of the HIE form, which does not fully cover the necessary medical records and documents and does not include detailed information on hospices, such as patient admission policies, service coverages, and current bed occupancies. Receiving the right care in the right place at the right time is vital to patients who are living their last few weeks or months [15]. To ensure their quality of life, the existing referral system must be strengthened.
There are precedent studies that have raised issues regarding the current HIE system, such as its usability, elements of the HIE form, and patient or guardian consent for sharing patient medical records [7]. These issues have been raised not only in Korea but also in other countries. Kisekka and Giboney [16] found that privacy concerns reduce the frequency of patient access to health records use and positive attitudes towards the HIE. However, belief in the effectiveness of information security increases the frequency of patient access to health records and helps to develop a positive attitude towards the HIE. Parker et al. [17] argued about the limited extent of data and lack of participation, which prevent further development of HIEs. Based on these studies, our study tried to provide insights into encouraging referrals of cancer patients to hospice facilities by suggesting a data model for collecting hospice facility information, a more adequate HIE form, and a re-design of the hospice referral for terminally ill cancer patients. However, there are many challenges to improving the existing referral system for cancer patients. Most of the hospice facilities have different patient admission policies and tend to deny admission to patients who need intensive care. Therefore, government-centered detailed guidelines and instrumentation requirements to admit patients to hospice care facilities are needed in the future. We expect our study to contribute by improving the quality of life of cancer patients, not only for the 10% of patients with cancer who are receiving hospice care presently but also for potential users in the future, by making the hospice referral system more efficient.